
The Morphological Stroke Risk Factors of PFO (MorPFO) Score
Background: It is still disputable whether the specific morphological properties of the patent foramen ovale (PFO) may contribute to the occurrence of stroke. Therefore, the aim of this study was to evaluate the differences in the morphometric and functional features of the PFO channel in cryptogenic stroke and non-stroke patients.
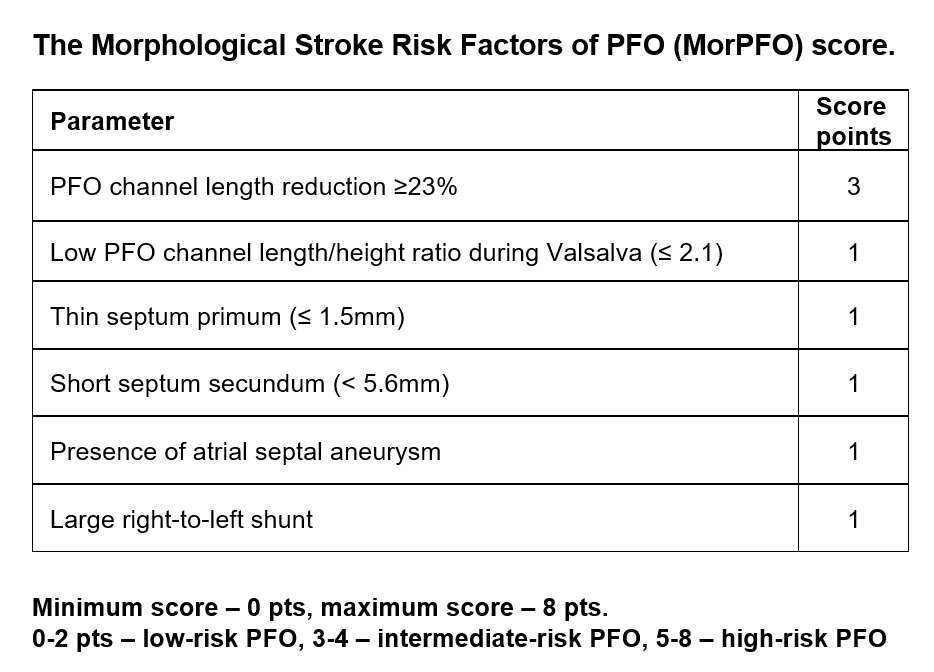
Methods and results: A total of 106 consecutive patients with cryptogenic stroke and 93 non-stroke control patients with diagnosed PFO (by transesophageal echocardiography) were analyzed. Multivariate regression logistic analyses indicated PFO channel length change (OR: 2.50 [95%Cl:1.75-3.55], p<0.001), the PFO length/height ratio during the Valsalva maneuver (OR: 0.75 [95%Cl:0.60-0.95], p=0.015), septum primum thickness (OR: 0.34 [95%Cl:0.14-0.80], p=0.013), septum secundum height (OR: 0.91 [95%Cl:0.84-0.98], p=0.013), the presence of an atrial septal aneurysm (OR: 3.38 [95%Cl:1.27-8.97], p=0.014), and large shunt (OR: 2.49 [95%Cl:1.13-5.46], p=0.022) as PFO-related risk factors for stroke. A MorPFO score was developed (AUC=0.816, SD=0.031), where six factors were included: PFO channel length reduction (≥ 23%) (3 pts), low length/height ratio during the Valsalva maneuver (≤ 2.1) (1 pt), thin septum primum (≤ 1.5mm) (1 pt), short septum secundum (< 5.6mm) (1 pt), presence of an atrial septal aneurysm (1 pt), and large right-to-left shunt (1 pt). Patients with scores of 0-2 pts had low-risk PFO channels, 3-4 pts intermediate-risk PFO channels, and 5-8 points high-risk PFO channels.
Conclusions: Transesophageal echocardiography can be used to determine the PFO-related risk of stroke. MorPFO score may help to identify high-stroke-risk PFO channels.
Powered by Eventact EMS