
Stent-Grafting via Unilateral Superficial Femoral Artery (SFA) Route for the Repair of Large-Bore Access Site Complications
Background: To safe use of a large-bore sheath, proper suture-based closure of the puncture site with modern closure device (VCD) is extremely important. In the case of VCD failure urgent hemostasis can be achieved using a contralateral delivered stent-graft, but this route takes time, skill and fortune. Our study demonstrates the feasibility of the completely unilateral stent grafting for the management of VCD failure.
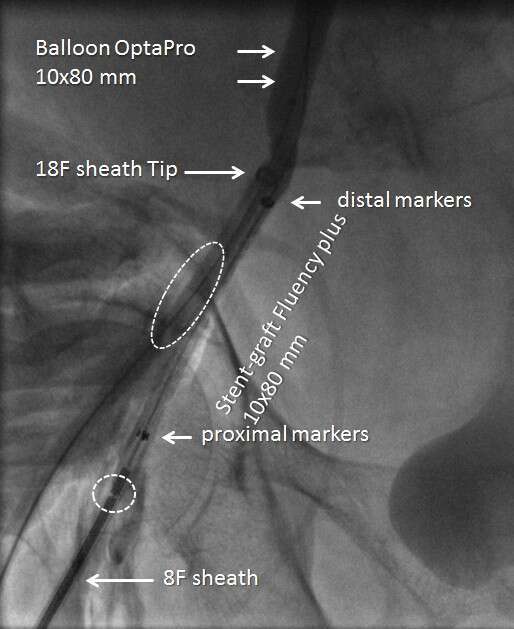
Methods: Eight cases of arterial access site complications developed during high-risk TAVI were studied. Complete hemostasis had not been achieved using either two PerClose (in 6/8) or ProStar XL (in 2/8). In two cases severe arterial rupture occurred. Unilateral stent-graft insertion through upper SFA was chosen because of complex iliac and aorta anatomy. During unilateral balloon inflation the SFA was punctured and the 8F introducer was advanced through the puncture site. "Fluency Plus" self-expandable stent-graft was implanted to cover the rupture site. (figure 1).
Results: Unilateral stent-graft delivery and implantation at proper femoral sites were successful in 100% cases, without further complications. in 2/8 cases we had a problem of parallel sheath insertion due to small CFA diameter and heavy calcification. This obstacle was overcome after the large sheath is withdrawn. In 6 cases the procedure was completed by the closure with "Angioseal" device, in two patients by manual compression. In 5 cases groin hematoma occurred during active extravasation. No vascular surgery and any additional interventions were required.
Conclusion: A prompt unilateral balloon-assisted hemostasis followed by stent-graft implantation is a feasible maneuver for repairing VCD failure.
Powered by Eventact EMS