
Long Term Outcome of Emergency Department Patients with Recent-Onset Atrial Fibrillation and Flutter
2Internal Medicine E, Emek Medical Center, Afula, Israel
3Bruce Rappaport Faculty of Medicine, Technion-Israel Institute of Technology, Haifa, Israel
Background
Atrial fibrillation (AF) is the most common arrhythmia among patients applying to the Emergency Department (ED). The current guidelines recommend choosing rate slowing agents (RSA) and or an antiarrhythmic therapy with not favor a particular treatment strategy. This study was conducted to determine the prevalence of adverse cardiovascular events as Stroke, Heart failure, Myocardial infarction and recurrence AF among the treatment strategies.
Methods
We conduct a retrospective observational study at Emek Medical Center, ED. Data was collected from June 2014 to June 2017.
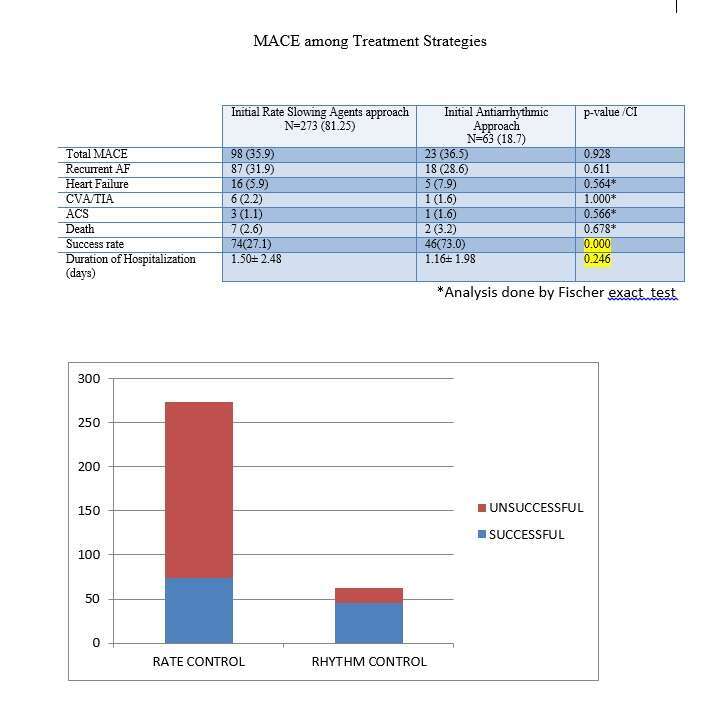
Results
The study included 344 patients. The most common initial treatment approach was rate slowing agents (79.4%) followed by antiarrhythmic therapy (18%). Spontaneous cardioversion was observed in 2.3% of cases. The highest success rates were observed after electrical cardioversion, followed by antiarrhythmic and RSA therapy (96.5%, 69.9%, and 25%, respectively). More than one-third (35.5%) of patients experienced at least one major cardiovascular event at one-year follow-up after being discharged from the hospital. Chronic kidney failure, heart failure (LVEF <40), Recurrent AF, COPD, and thyroid dysfunction were found to be variables that affect the prevalence of MACE rate. Patient who had more than one episode in the past year had fewer MACE events when antiarrhythmic therapy and / or electrical cardioversion was applied as first strategy compared to RSA therapy (p <0.003). The proportion of patients admitted and the duration of hospitalization in this group of patients was significantly lower. In patients who have been first diagnosed with AF or who have not experienced frequent AF in the past year, treatment initially with RSA seems, though not significantly, a better therapeutic strategy.
Conclusion
Initial treatment strategy applied in ER seems to affect outcome. Patients with non-permanent AF and frequent recurrences in the past year will benefit from fewer MACE events, lower hospitalization rate, and shorter hospitalization length after initial antiarrhythmic treatment and prompt cardioversion.
Powered by Eventact EMS