
Kawasaki Disease with Gallbladder Hydrops: An Atypical Presentation in a 3-month-old Infant
Background: Diagnosing atypical Kawasaki disease can be a challenge, and due to rarity of this disease in infants, this challenge is augmented. Missed cases or delayed treatment can lead to serious complications. We are reporting an infant of 3 month old with atypical Kawasaki presentation.
Case summary: 3 month old male infant presented with fever, vomiting and diarrhea of four days duration. He also had bilateral non-purulent conjunctivitis, marked irritability, BCG site reactivation and no other symptoms with no history of contact with sick patients.
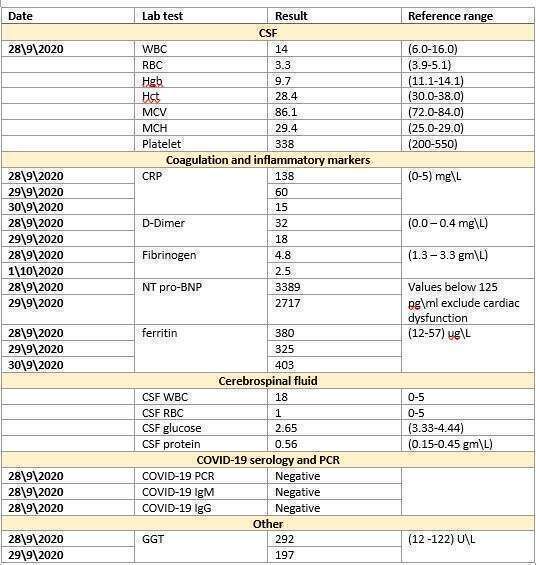
Partial septic work up done in the emergency and started initially on cephalosporin with still spiking high grade fever. In the floor he still had the same symptoms so full septic workup done after starting Antibiotic by 4 days , DIC panel, CRP, pro-BNP, ferritin in which all were high (table -1).
Due to tender liver during examination GGT order which was high and US abdomen showed distended Gall Bladder with wall thickening suggestive of hydrops of the gallbladder.
Pediatric rheumatology consulted and advice for ECHO and start intravenous immunoglobulin and aspirin as diagnose of Kawasaki. Echocardiography showed normal coronary artery.
The patient was given on dose of intravenous immunoglobulin 1 gm\kg, started on methyl prednisolone 1mg\kg for 5 days, and aspirin. He also received 14 days of cephalosporin. Fever has resolved after the fourth day, as well as the other symptoms. The patient was discharged with a follow up echo after 2 weeks while kept on aspirin.
Conclusion: Children with incomplete Kawasaki disease often remain undiagnosed for several days, therefore they are at a greater chance of developing coronary artery abnormalities. Persistent fever with no improvement should alert clinicians to Kawasaki disease diagnosis specially in this age group and treat without a delay to avoid serious complications.
Powered by Eventact EMS