
Baccille Calmette – Guerin (BCG) Vaccine Induced Osteomyelitis in Immunocompetent Children
2Clinic of Children’s Diseases, Vilnius University, Institute of Clinical Medicine, Vilnius, Lithuania
3Department of Pediatric Surgery, Lithuanian University of Health Sciences, Medical Academy, Kaunas, Lithuania
4Pediatric Department, Lithuanian University of Health Sciences, Kaunas Hospital, Kaunas, Lithuania
Background: BCG-induced osteomyelitis is an extremely rare systemic adverse reaction after BCG vaccination in immunocompetent children, and the correct diagnosis is frequently missed.
Objective: To highlight management features of BCG bone lesions in order to avoid delays in a diagnosis.
Methods: Retrospective analysis was made of the medical data of children who had BCG osteomyelitis diagnosed over a ten-year period.
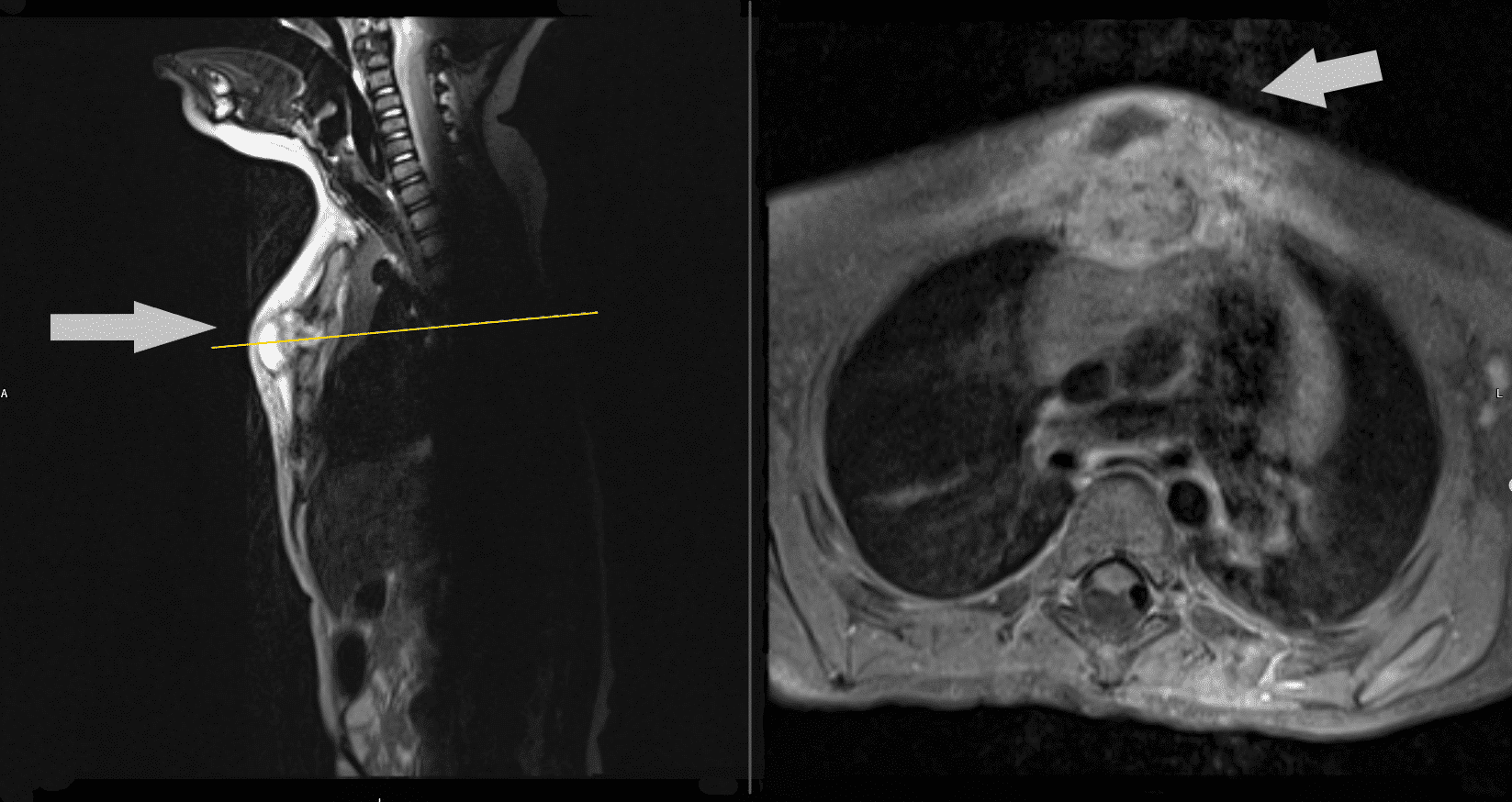
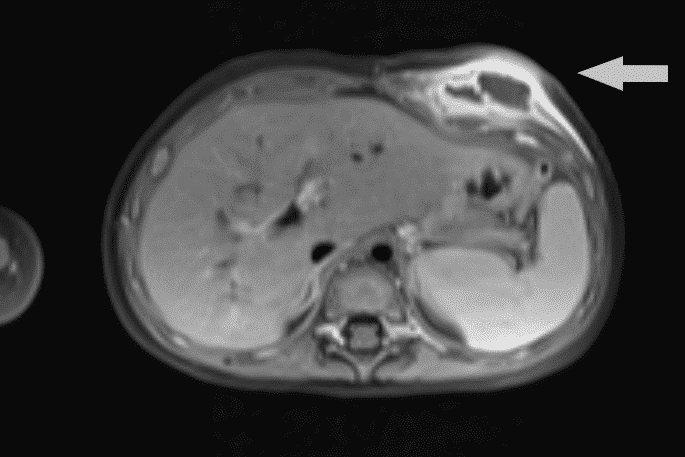
Results: BCG bone lesions were observed in three boys and one girl, occurring between 9-16 months after vaccination. We report a considerably higher BCG osteomyelitis incidence rate-12.3 per million BCG vaccinated children in Lithuania. Two patients received the Japanese type of BCG while the other two received Danish and Bulgarian types, respectively. Three cases of BCG chest bone osteomyelitis (Fig 1) and one case of BCG femoral lesion were observed between 2008 and 2018. Limping was the only symptom in the patient with femoral lesion. Ultrasonography, computed tomography and magnetic resonance imaging tests were nonspecific and showed destruction or inflammation of the affected area (Fig 2, 3, 4). Histological and microbiological tests were the main diagnostic tools for the confirmation of diagnosis. Necrotic granuloma was found in three cases. Acid-fast bacilli were found in two cases, and the M.bovis BCG strain identified by genotyping-TB method was confirmed in three cases. One of the patients did not have bacteriological confirmation, but tuberculin skin test was “hyperergic” without evidence of latent TB infection. QuantiFERON-TB tests were negative in three cases and not available in one. All children were verified as immunocompetent. Surgery was performed in all cases and anti-TB drugs were prescribed individually. All patients with BCG-induced bone lesions were successfully treated with anti-TB drugs.
Conclusions: BCG osteitis should be considered in all vaccinated children with atypical bone lesions of unknown origin. Early biopsy of the lesions can protect against diagnosis delay.


Powered by Eventact EMS