
Force Biomechanical Evaluation of a Back Handspring of a Patient in a SLAP Type II Injury Rehabilitation
2McGill University, Quebec
3Biomexanik, Mexico City
4Universidad Autónoma de México, Mexico City
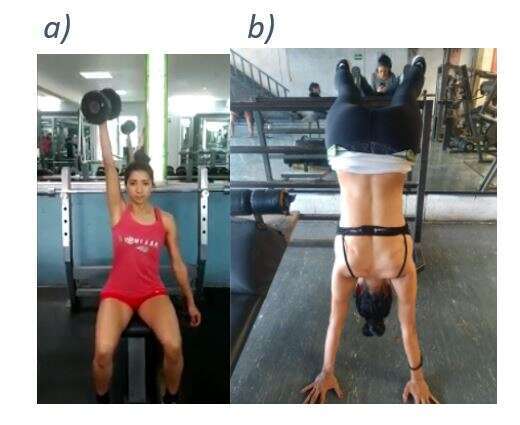
Introduction: Back Handspring is one of the most important backward elements in gymnastics. The technique can be divided into 3 phases: (1) unbalanced take-off, (2) flight, and (3) maximal acceleration (Gutiérrez Vélez & Estapé Tous, 2001). At phase 1, both arms generate a humeral flexion at maximum velocity, from the sides of the trunk to above the head. The shoulder becomes vulnerable due to the ground impact and the excessive range of movement above the head.
Superior labral anterior to posterior (SLAP) lesion is usually found in athletes with high arm overhead activity (Valero González & Inzunza Enríquez, 2016). SLAP injuries are classified into several types depending on the place where the tear occurs. However, type II has been reported to be the most common injury of overhead athletes (Manske & Prohaska, 2010).
There are no quantitative criteria to monitor the relation between force generated by the athlete during shoulder flexion and back handspring, and therefore no criteria to indicate when the athlete is ready to start training.
Aims: To develop a biomechanical exercise protocol for monitoring maximal isometric and explosive force of a patient suffering SLAP II tear, and to improve movement symmetry of both arms during a back handspring.
Methodology
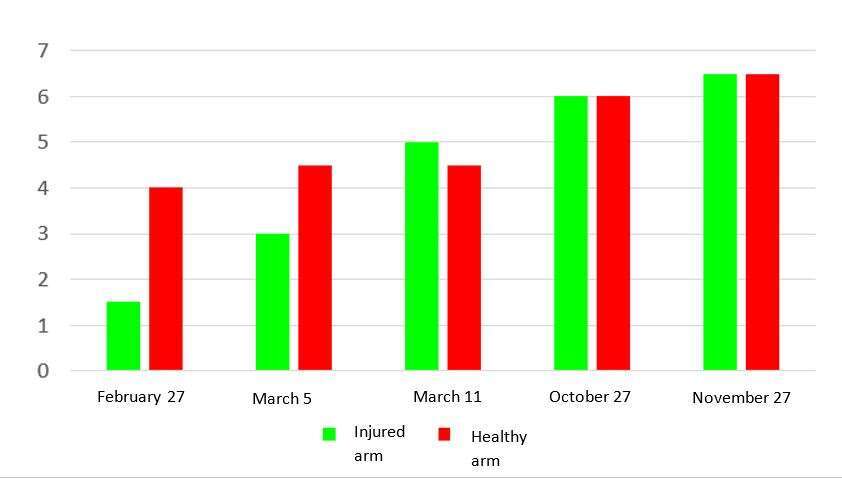
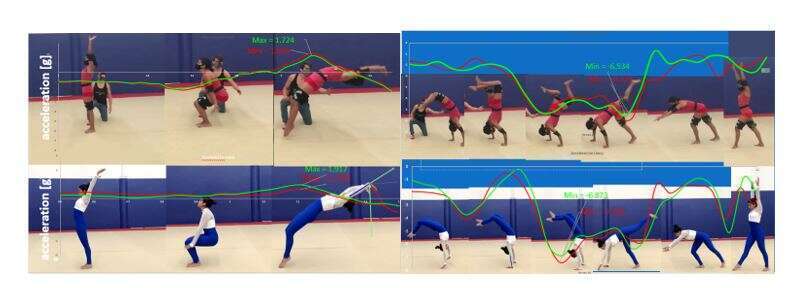
Methods: A patient diagnosed with SLAP II tear was treated for a year (from January 2020 to November 2020) to recuperate shoulder range of movement and humeral flexion from 0 to 180 degrees. After recovering glenohumeral stability, a physical preparation program was developed. All exercises were initially done with no or low weight, with progressively added weight and repetitions. Articular biomechanics evaluations were done to detect differences of force generated by the injured and healthy shoulders. The duration of the physical preparation program was 10 months. Motion capture data of back handspring was collected using three inertial sensors (mBientLab MMR).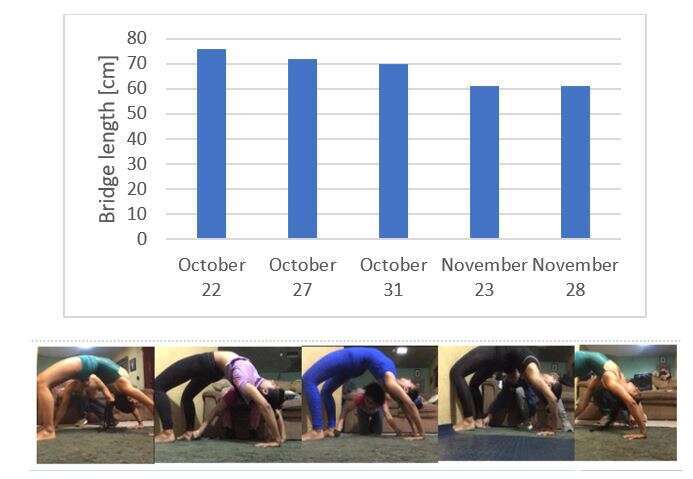
Results: At the beginning the patient was unable to do a 180° shoulder flexion, and therefore was unable to perform an arch or a back handspring (Figure 2). At the end of the program the patient recovered full range of movement of the shoulder and was able to perform a back handspring again.
Discussion: During a full year of rehabilitation, the patient recovered enough shoulder range of movement and stability to perform a back handspring again. The protocol used in this research was successful in taking the athlete back to normal sport activity. Due to Covid-19 circumstances, the patient was not able to use specialized equipment for the rehabilitation. It is concluded that the progress would be faster if specialized equipment, such as a variety of weights, could be used.

Powered by Eventact EMS