
Guideline recommended therapies and clinical outcomes in patients with particularly high-risk for recurrent cardiovascular events after an Acute Coronary Syndrome-
The ACSIS registry
2Sackler Faculty of Medicine, Tel Aviv University, Israel
3Cardiac Research Institute, Sheba Medical Center, The Israeli Center for Cardiovascular Research (ICCR), Israel
Background: Patients with ACS are at increased risk for recurrent CV events, but some patients, such as the elderly and with prior comorbidities are at the highest risk. We examined temporal trends in the management and outcomes across the spectrum of this particularly high-risk group.
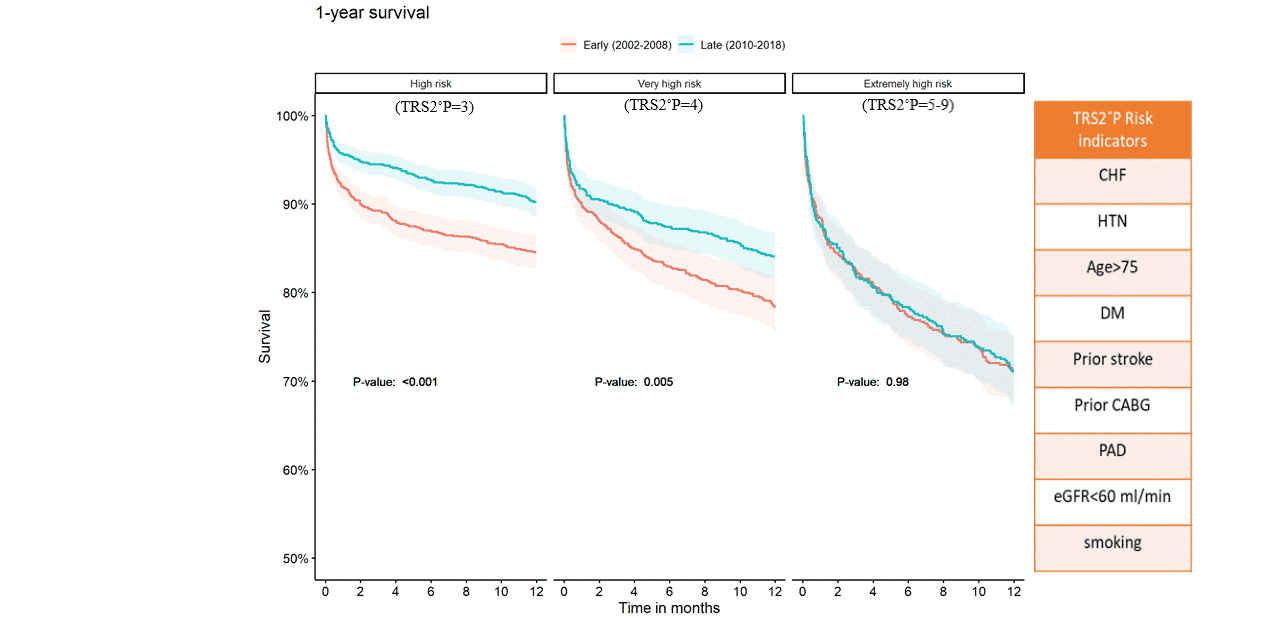
Methods: Data from the acute coronary syndrome Israeli survey (ACSIS) registry. Patients were stratified according to the TIMI risk-score for secondary prevention (TRS2˚P) to high (TRS2˚P=3), very high (TRS2˚P=4), or extremely high-risk (TRS2˚P=5-9). Clinical outcomes included 30-day MACE and 1-year mortality. Temporal trends were examined in the early (2002-2008) and late (2010-2018) time-periods.
Results: Among 5,359 patients (50% high-risk, 30% very high-risk, and 20% extremely high-risk), those with a higher-risk were older, had more comorbidities, presented more with NSTEMI, and were treated less with guideline-recommended pharmacotherapy and PCI. During time, treatment has improved in all risk-strata, and the rate of 30-day MACE has significantly decreased in all risk groups (21% to 10%, 22% to 15%, and 26% to 16%, in high, very high, and extremely high-risk groups, P<0.001 for each). However, 1-year mortality decreased only among high and very high-risk patients but not among extremely high-risk patients in whom 1-year mortality rates remained very high (28.7% vs. 28.9%, P=1).
Conclusion: Within a particularly high-risk cohort of patients with ACS, treatment has significantly improved over almost 2 decades. While short-term outcomes improved in all risk-groups, 1-year mortality improved only in the high and very high-risk groups.
Powered by Eventact EMS