
The association of tissue doppler E/e` ratio with poor survival is modified by gender and is attenuated with advanced age
Introduction: Contemporary guidelines recommend a universal cutoff of 14 for the ratio between early mitral flow wave and early diastolic mitral annulus velocity measured by tissue doppler (E/e’ ratio). While age-dependent normal E/e’ values have been suggested, outcome data is lacking.
Methods: Consecutive patients who underwent echocardiographic evaluation during 2009-2021 (N=104,315) in a single tertiary cardiovascular center. Patients with left or right ventricular dysfunction, any significant valvular disease, structural heart disease or evidence of pulmonary hypertension were excluded. Patients with a metastatic malignancy at baseline or follow up were excluded.
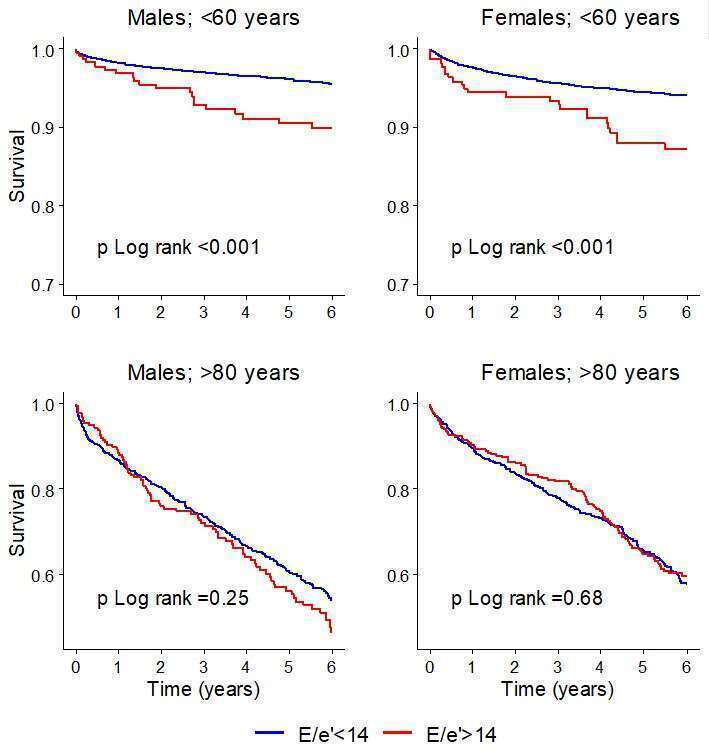
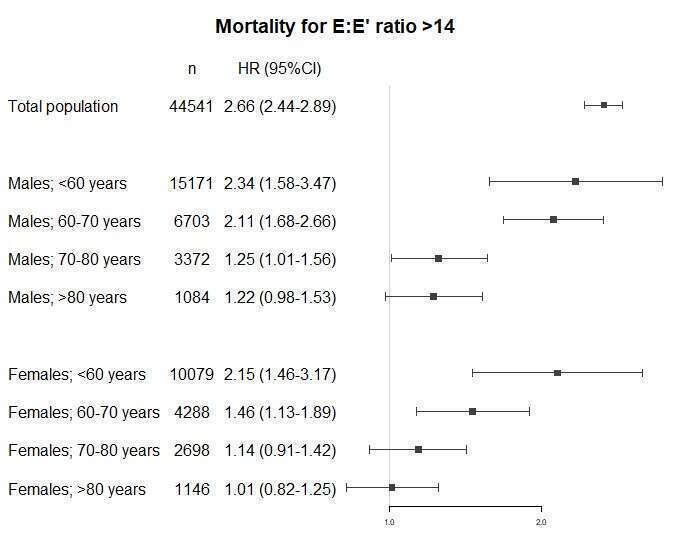
Results: Overall, 44,541 patients were included in the final analysis. Mean age was 55±17, 59% were male and 63% of the exams were performed in an outpatient setting. An E/e’>14 was documented in 2,598 (7%) patients. During a median follow-up of 5.7 (IQR 2.8-9.1) years, 5,015 (11.3%) patients died. Kaplan Meier survival analysis demonstrated that the cumulative probability 6-year mortality was 23.4% (21.6-25.3) among patients with E/e`>14, compared with 9.7% (9.3-10.0) among patients with E/e`<14 (p Log-rank <0.001). This difference was less significant as age progressed (figure 1). Multivariate cox-regression model yielded consistent results such that an elevated E/e’ ratio was associated with 2.66-fold increased risk of death during follow up (95%CI 2.44-2.89, p<0.001), and there was a decline in the increased risk as age advanced in both genders (figure 2). Interaction analysis was significant for both gender and age such the association of elevated E/e` ratio with poor survival was more significant among men compared with women and among young vs. older subjects.
Conclusion: In apparently normal hearts, an elevated E/e’ ratio is independently associated with increased mortality. This association is more pronounced among men and is attenuated with increased age. This study supports the need for gender-specific and age-specified outcome data with respect to measures of diastolic dysfunction.
Powered by Eventact EMS