
Clinical and echocardiographic parameters associated with left ventricular recovery after TAVI
2Sackler Faculty of Medicine, Tel-Aviv University, Israel
Introduction: The relationship between severe Aortic Stenosis (AS) and Left Ventricular (LV) dysfunction is well established. However, there is a paucity of data regarding LV functional recovery after TAVI.
Methods: We evaluated all patients who underwent TAVI between 2009-2020 in a tertiary hospital. We included patients with pre-procedural LV Ejection Fraction (LVEF) of 40% and below. All patients had baseline and in-hospital post-procedural echo, and their clinical characteristics were recorded in a designated TAVI registry. LV functional recovery was defined as an absolute increase in at least 10% in LVEF post-procedurally. No LV recovery was defined as an absolute change of up to ±10% in post-procedure LVEF. Univariate analysis consisting clinical and echocardiographic factors for LV functional recovery was performed, followed by logistic regression adjusting for confounders.
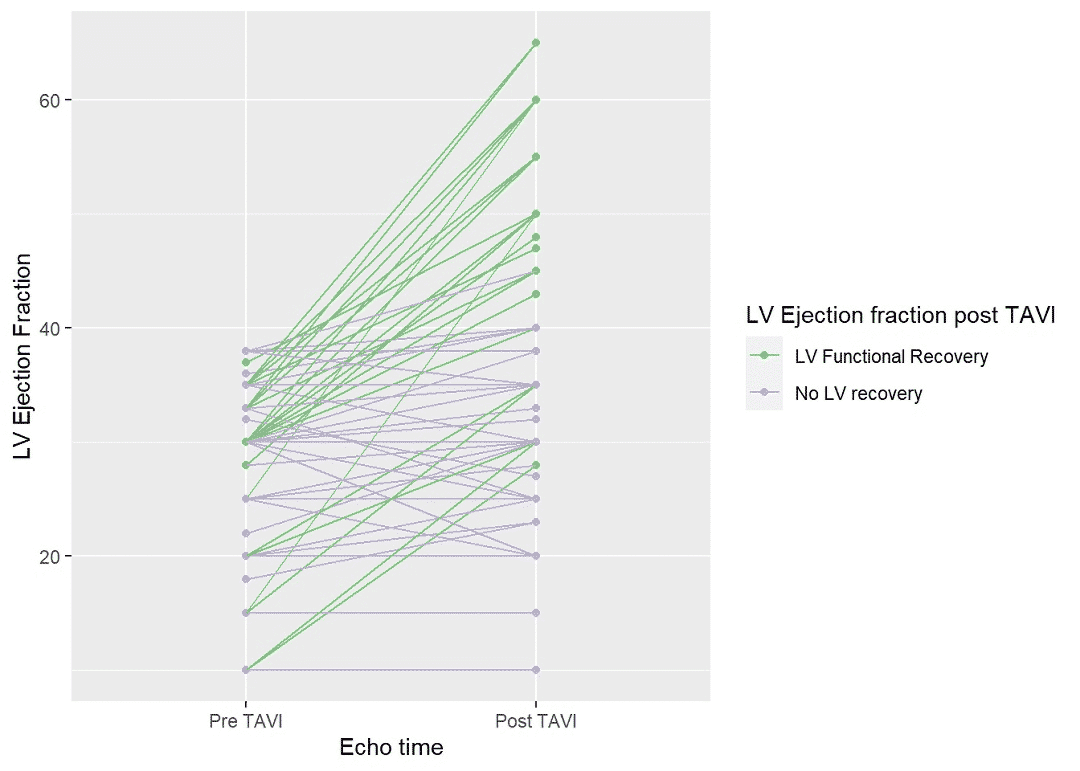
Results: Out of 1,349 consecutive TAVI patients, 100 (7.4%) had LVEF of 40% or less. There were 69 (69%) men with a mean age of 82±8 years, and average BMI of 27±4 kg/m2. Out of these 100 patients, 32 (32%) had achieved LV functional recovery and no patient had experienced LVEF deterioration (FIGURE). Mean Left Ventricular End Systolic Diameter (LVESD) was 3.79 and 4.43 in the LV functional recovery and no LV recovery groups, respectively. Mean aortic pressure gradient was higher among patients who had LV functional recovery compared to no LV recovery (45.9 vs. 31.5 mmHg, respectively). Multivariable analysis revealed parameters that were independently associated with LV functional recovery: Coronary artery disease - OR 5.29 (95%CI 1.59-20.44), LVESD - OR 0.87 (95%CI 0.8-0.95) for each 1 mm and mean aortic pressure gradient – OR 1.91 (95%CI 1.21-3.28) per each 10 mmHg.
Conclusion: In patients with severe AS and LV dysfunction undergoing TAVI, the presence of coronary artery disease, increased aortic pressure gradient and reduced LVESD were associated with early LV functional recovery.
Powered by Eventact EMS