
Usefulness of serial six-minute walk test in ambulatory heart failure patients
Introduction
The 6MWT (6-minutes walk test) is an easy and safe sub-maximal test for functional capacity. A single test was found to be a good prognostic marker for HF morbidity and mortality. However, 6MWT results may change during the ambulatory course. We examined repetitive 6MWT in ambulatory HF (heart failure) patients for variance, trends, and correlation with clinical outcomes.
Material and method
The 6MWT is done routinely in our HF clinic. Patients who had ≥3 6MWD (6-minutes` walk distance) measurements were included. For each patient`s 6MWTs, ratio between current distance to median of all previous tests was pooled. Total ratio for each patient was defined as the mean of all ratios. Patients were considered to deteriorate function if the total ratio was below 0.95.
Results and discussion
For 377 patients (mean(±SD) age 65.9±15 years, 29.4% females, 52% with EF<40%, median 6MWT measurements per patient was 7[4-10]. Overall 6MWD improved between HF clinic visits but with significant individual variability (Figure 1). The total 6MWD ratio distributed normally: mean (±SD) 1.07±0.21. There were 75(19.9%) patients that overall worsened 6MWD (total ratio<0.95). During median follow up of 978[591-1516] days, crude mortality rate was 13.5%. Worsened patients` mortality was higher (25.3% vs 10.6%) (p<0.001). Using the multivariable cox model including baseline 6MWD, number of tests, age, gender and reduced LV function - overall 6MWD deterioration by > 5% was independently associated with increased mortality rate (HR=2.53 95%CI [1.29-4.98] p=0.007) (Figure 2).
Conclusion
Overall deterioration in 6MWD was associated with poorer outcomes, supporting the prognostic value of repetitive 6MWT measurements over a single test.
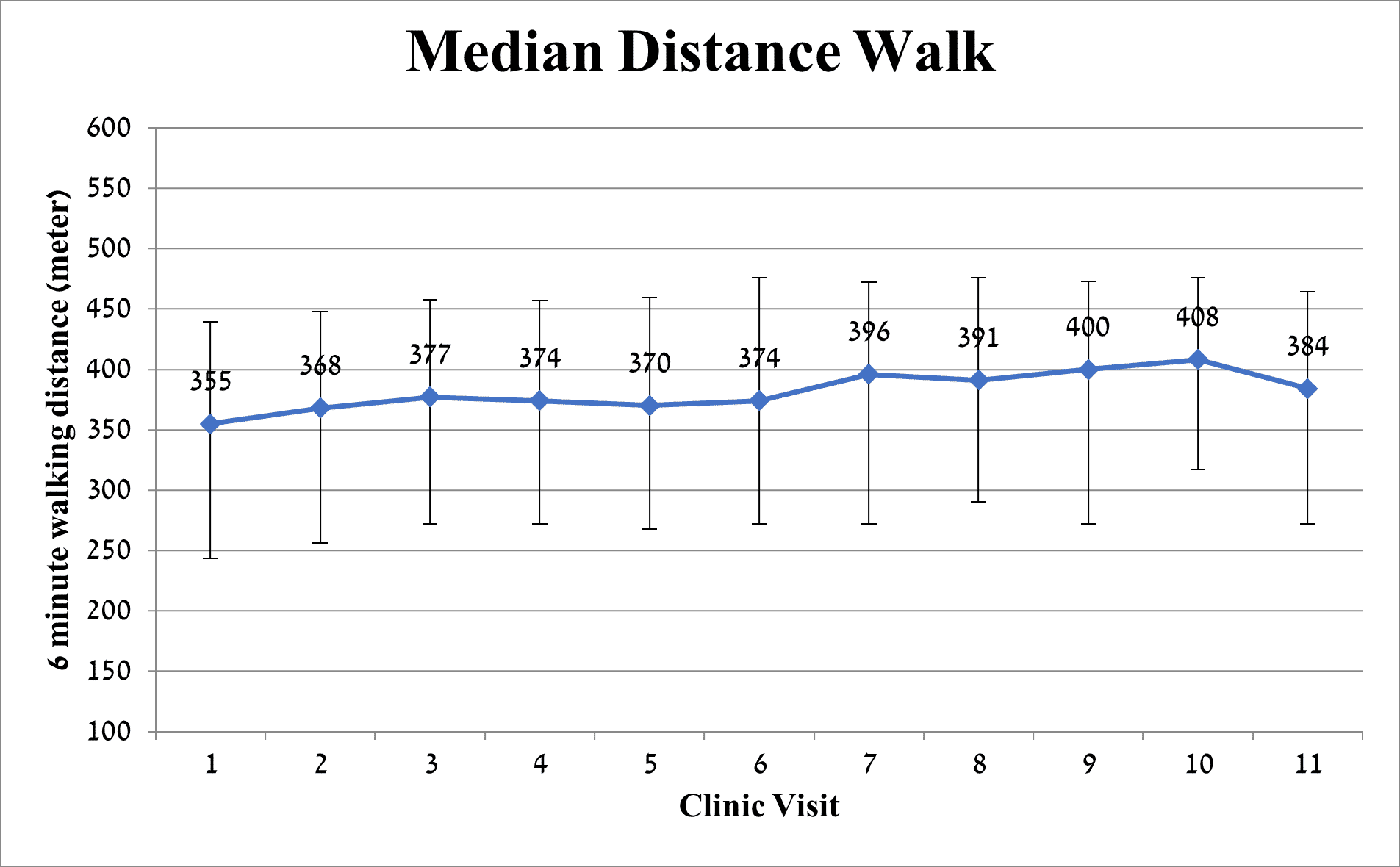
Figure 1 – Median distance walk with IQR
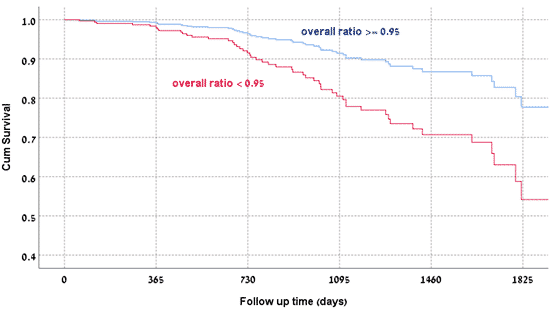
Figure 2
Powered by Eventact EMS