
Reproducibility of Echocardiographic Techniques for Assessment of Ventricular Function
2Cardiac Arrhythmia Research Laboratory, Department of Physiology and Cell Biology, Faculty of Health Sciences, Ben Gurion University, Israel
3Cardiology Department, Soroka University Medical Center, Israel
Introduction: Sequential assessment of ventricular function by echocardiography is used in a variety of conditions. Ventricular function is monitored by ejection fraction (EF) and global longitudinal strain (GLS). Precision (inter-observer variability) in calculation of EF and GLS is a disadvantage of the echocardiographic follow-up. We aim to assess the inter-observer variability of different methods that evaluate cardiac function in our echocardiography lab.
Material and methods: EF was assessed by 2D using an automatic border detection program (EFI) and GLS by AFI (Vivid E95); both programs allow manual correction of the region of interest. A second assessment of EF and GLS was performed using the same echocardiography study by an echocardiographer, unaware of the previous results. The difference between the two analysis was calculated by extraction, and patients were separated into low (EF<50%, AFI<18) and normal (EF≥50%, AFI≥18) by the mean of the two results.
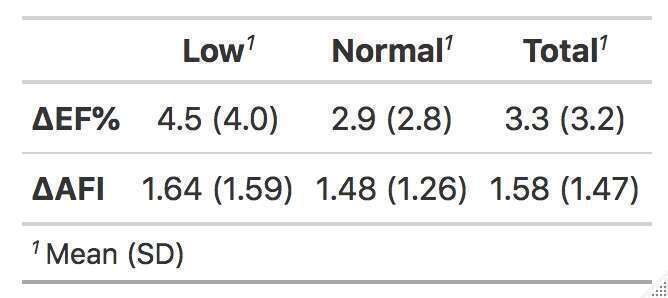
Results and discussion: Sixty-nine patients, 62% males, aged 56 ± 9 years were evaluated. The results are depicted in the Table1. In patients with low EF and low GLS the variability was higher than in those with normal EF and GLS. There were 13/69 (18.8%) patients with a delta EF% > 5 between observers and 2/69 (2.9%) > 10%. There were 18/69 (26.1%) patients with delta GLS > 2 and 1/69 (1.4%) > 5. The major restriction of this study is that analysis was performed from the same recording, rather than a new assessment of LV function by a second technician, isolating the variability on the analysis rather than image acquisition.
Conclusion: A change greater than 10% in EF%, or greater than 5 in AFI during patient follow-up should be seriously considered. GLS is a more precise and consistent parameter for the assessment and follow up of LV function in comparison with EF%.
Powered by Eventact EMS