
Evolution of right and left ventricle routine and speckle-tracking echocardiography in patients recovering from coronavirus disease 2019 – a longitudinal study
2Faculty of Health Sciences, Ben-Gurion University of the Negev, Israel
3Department of Intensive Care, Tel Aviv Sourasky Medical Center and Sackler School of Medicine, Tel Aviv University, Israel
4Department of Paediatrics, Paediatric Cardiology Unit, Tel Aviv Sourasky Medical Centre and Sackler School of Medicine, Tel Aviv University, Israel
5Department of Paediatric Cardiology, Amalia Children’s Hospital, Radboud University Medical Centre, Netherlands
Background: Data on systematic longitudinal assessment of cardiac imaging in patients recovering from Coronavirus disease 2019 (COVID-19) infection is limited.
Methods: Routine comprehensive echocardiography and STE of both ventricles were performed during hospitalization for acute COVID-19 infection as part of a prospective pre-designed protocol, and compared with echocardiography performed approximately three months post recovery in 80 patients, using a similar protocol.
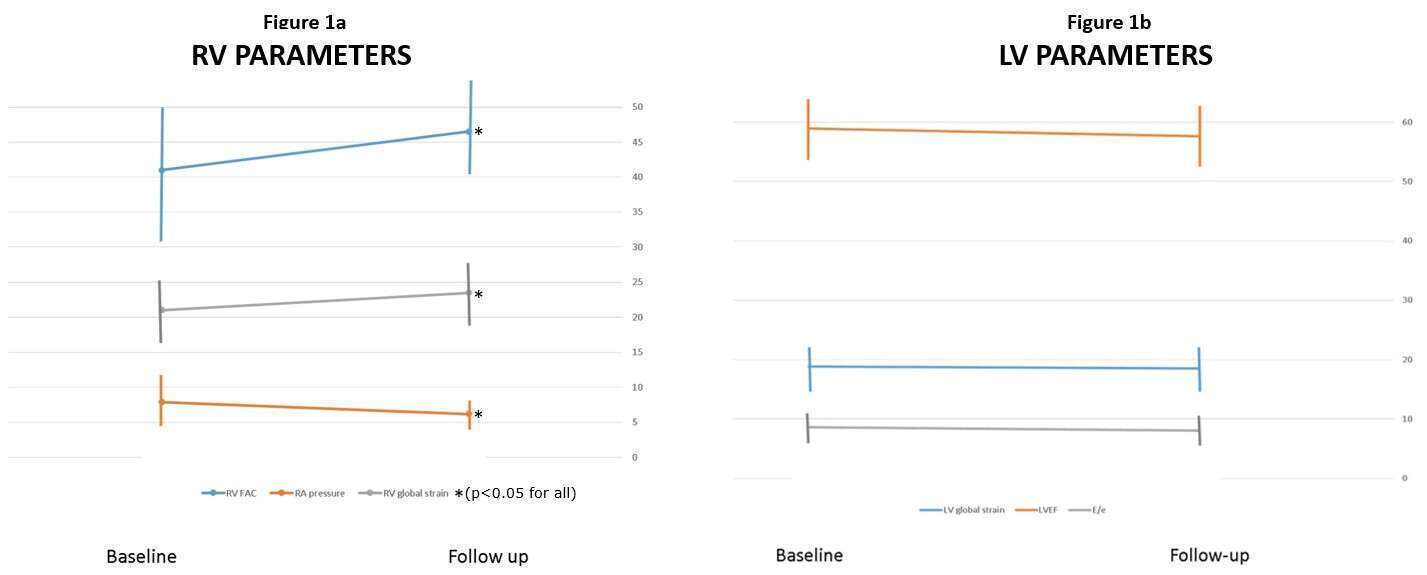
Results: Significantly improved right ventricle (RV) fractional area change, longer pulmonary acceleration time, lower right atrial pressure, and smaller RV end-diastolic and end-systolic area were observed at the recovery assessment as can be seen in Figure 1a (p<0.05 for all). RV global longitudinal strain improved at the follow-up evaluation (23.2±5 vs. 21.7±4, p=0.03), mostly due to improvement in septal segments. Only 8 (10%) of patients recovering from COVID-19 infection had ejection fraction (EF) <50% at follow-up. However, LV related routine (E, E/e, stroke volume, LV size), or STE parameters did not change significantly from the assessment during hospitalization as can be seen in Figure 1b. A significant proportion (36[45%]) of patients had deterioration of longitudinal strain at follow-up, and 19 patients (24%) still had abnormal LV STE approximately three months post COVID-19 acute infection.
Conclusions: In patients previously discharged from hospitalization due to COVID-19 infection, RV routine echocardiographic, and RV STE parameters improve significantly concurrently with improved RV hemodynamics. In contrast, a quarter of patients still have LV systolic dysfunction based on STE cutoffs. Moreover, LV STE does not improve significantly, emphasizing the importance of STE analyses in the evaluation of patients recovering from COVID-19 infection.
Powered by Eventact EMS