
Outcomes of patients admitted with high-sensitive cardiac troponin t levels meeting the new rule out criteria for myocardial infarction
2Department of Internal Medicine B, Rabin Medical Center, Israel
3Cardiology Institute, Shamir Medical Center, Israel
4Biochemistry and Pharmacology Laboratory, Rabin Medical Center, Israel
5Clinical Laboratories, Rabin Medical Center, Israel
Background: The 2020 ESC non-ST-elevation (NSTE) acute coronary syndromes (ACS) guidelines have adopted the paradigm that patients presenting with suspected NSTE-ACS and high-sensitive cardiac troponin T (hs-cTnT) values <99th percentile in a single test or small increment within 1/2 hours have a high negative predictive value for myocardial infarction (MI). Their management remains controversial.
Purpose: We examined the clinical outcomes and resource utilization of suspected NSTE-ACS patients who presented with hs-cTnT values meeting the early rule out criteria, but were nevertheless admitted.
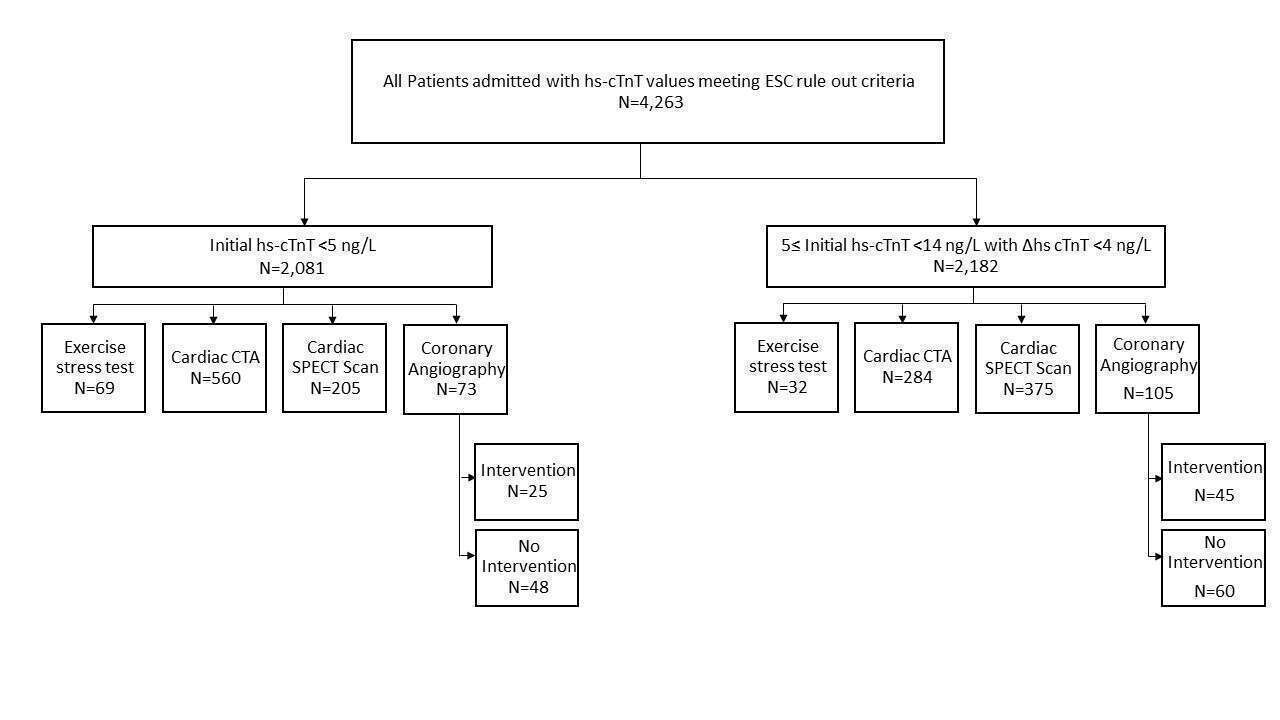
Methods: Our single center retrospective cohort study included 4,263 visits for suspected NSTE-ACS triaged in the Emergency Room (ER), had hs-cTnT values that met the early rule-out criteria, and were admitted (Figure).
Routine quality control and dedicated tests proved a coefficient of variance of <10% for hs-cTnT values < 99th percentile (14 ng/L).
Results: There were no deaths in-hospital and at 30 days. Discharge diagnosis of MI was documented in 10 patients (~0.2%). Median ER stay and hospital stay were 6 hours and 3 days, respectively. In hospital evaluation included 844 gated cardiac CT angiography, 580 SPECT heart scan, 101 ECG-exercise tests, and 178 coronary angiographies, of which 70 (~1.6% of cohort) culminated in percutaneous/surgical intervention.
Conclusion: Our findings highlight the high negative predictive value for MI applying the early rule out algorithm and supports a policy of ER discharge for further evaluation, sparing unnecessary and resource-consuming hospital admissions.
Powered by Eventact EMS