
Mild renal dysfunction among healthy adults is associated with remote incidence of atrial fibrillation
2Sackler Faculty of Medicine, Tel-Aviv University, Israel
3Institute for Medical Screening, Sheba Medical Center, Israel
4Institute of Nephrology and Hypertension, Sheba Medical Center, Israel
5Internal Medicine Wing, Sheba Medical Center, Israel
Introduction: The relationship between atrial fibrillation (AF) and advanced chronic kidney disease is well established. However, there is a paucity of data regarding the long-term association in between renal function and incidence of AF.
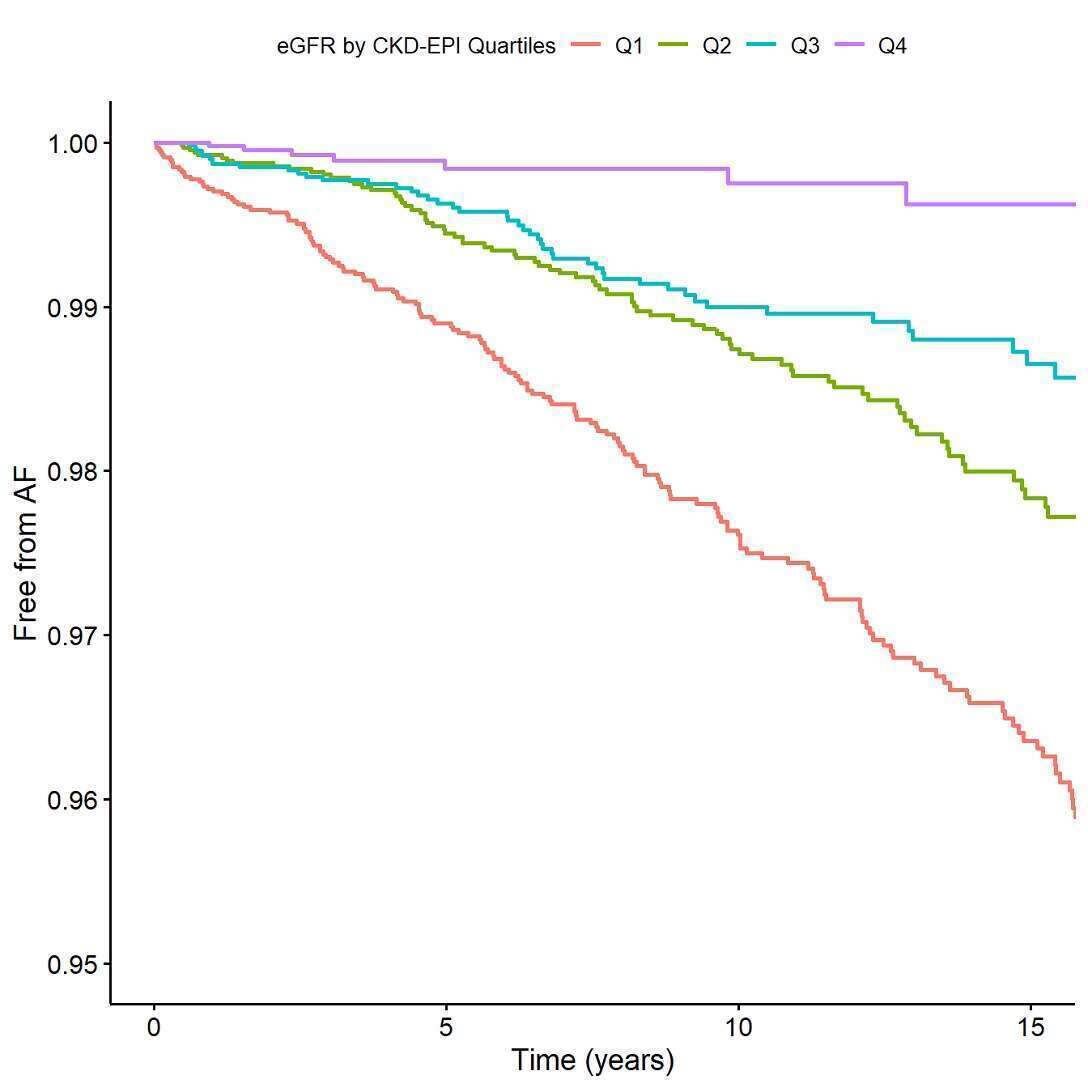
Methods: We evaluated asymptomatic self-referred adults who participated in a medical screening program. All subjects were free of AF at baseline. Estimated Glomerular Filtration Rate (eGFR) was calculated by CKD-EPI and divided into quartiles (Q1 represents the lowest quartile). Study endpoint was the development of AF which was externally adjudicated by a physician. Cox regression models were applied while adjusting for confounders.
Results: The final study population included 27,647 subjects (68% men) with a mean age of 47 years. At baseline (first screening visit), median eGFR by CKD-EPI was 84 [IQR 74;95] and 86 [IQR 74.;101] mL/min per 1.73m2 for men women, respectively. During median follow up of 7 years [IQR 2;14], 328 (1%) of subjects developed AF, of whom 271 (83%) were men and 57 (17%) were women. The incident AF eGFR distribution by quartiles was: 179 (55%%), 92 (28%), 50 (15%) and 7 (2%) subjects from eGFR Q1-Q4, respectively. Kaplan Meier survival analysis demonstrated a graded increased risk of AF with decreasing eGFR quartiles (p Log rank <.001; FIGURE). Multivariate cox regression analysis revealed hazard ratio of 2.76 (95%CI 1.26, 6.04), 3.05 (95%CI 1.31, 6.63), and 2.71 (1.23, 6.00) for AF incidence for Q1-Q3, respectively (using Q4 as reference).
Conclusion: Mild renal dysfunction even within the normal range is independently associated with remote risk of AF among young apparently healthy adults. Screening for AF should be considered among young patients with reduced renal function, even within normal reference range.
Powered by Eventact EMS