
Revascularization and urgent AVR in acute coronary syndrome setting (senior physician accompanying the case: Dr. Amos Levi)
A 64-year-old patient with a past medical history of dyslipidemia, hypothyroidism, and pre-diabetes.
The patient reported 4 months of typical angina but sought medical evaluation for the first time a month before her admission. An ambulatory echocardiogram two weeks before admission demonstrated moderate to severe aortic stenosis with preserved LV function.
Finally, the patient presented with acute MI and acute decompensated heart failure (Wet & Warm). Initial management demonstrated new LBBB on ECG and severe LV dysfunction secondary to infero-postero-septal contraction disorder and severe aortic stenosis on echocardiography.

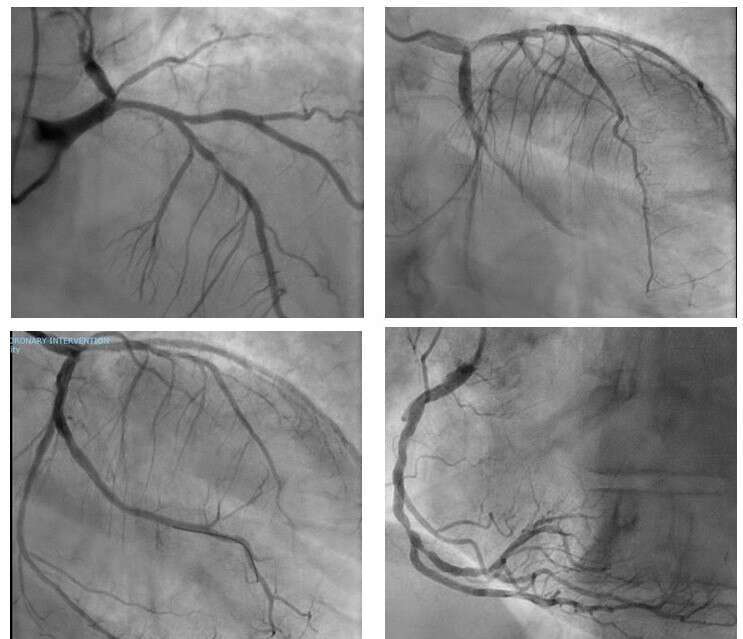
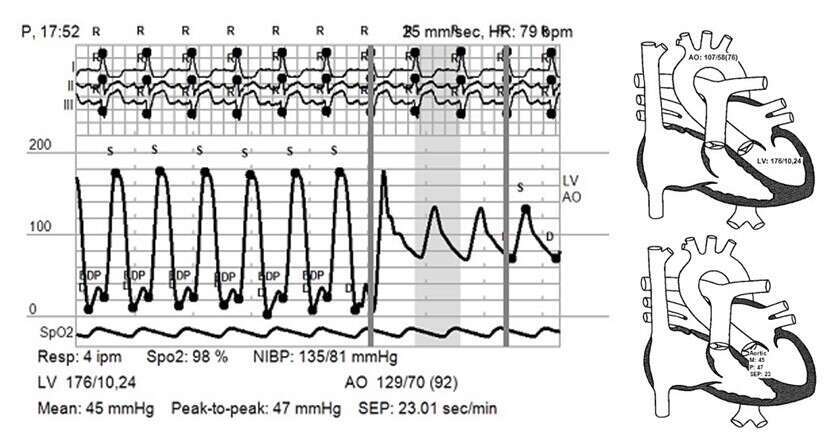
The patient was managed with primary PCI to the circumflex artery. Significant LAD and RCA disease were left for future intervention. The pressure gradient on the aortic valve confirmed severe AS. A short while after the revascularization, the patient developed a cardiogenic shock. Urgent echocardiography ruled out mechanical complications. The patient was stabilized and transferred awake to the ICCU supported by noradrenaline and IABP.
The next day the patient demonstrated a marked improvement. Following weaning IABP, a repeat echocardiogram demonstrated moderate to severe LV dysfunction and severe AS.
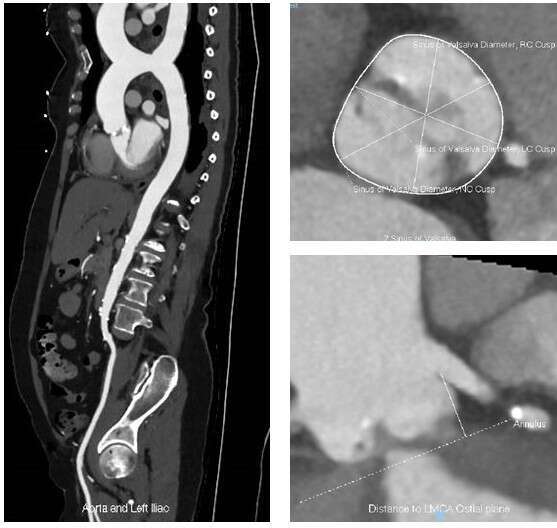
Further evaluation included TAVI protocol cardiac CTA demonstrated a heavily calcified bicuspid aortic valve.
A heart team considered the patient`s profile – her young age, bicuspid AV stenosis, and remaining coronary disease. It determined CABG and AVR were preferable to TAVI and staged PCI. STS Mortality Score of 7.7% and residual SYNTAX Score of 15 were calculated.
The patient continued DAPT based on aspirin and clopidogrel until the day of surgery. On the 8th day of hospitalization, the patient underwent CABG and surgical AVR.
Therapeutic dilemmas: management of a complex patient with STEMI, 3 vessels coronary disease, and severe valvular disease/ Consideration pro and against TAVI after primary PCI/ Preferred time interval between STEMI and CABG with/without surgical AVR/ Preferred peri-procedural anti-platelets strategy?
Powered by Eventact EMS