Background. Bevacizumab generally brings about an initial substantial radiologic response in most patients with glioblastoma (GB). Yet, several studies have shown that following bevacizumab, GB is more likely to progress to an infiltrative pattern, associated with an increased MRI T2-weighted signal1-4. This work aimed to study tumor progression in patients with GB undergoing bevacizumab therapy, by classifying the non-enhancing hyperintense T2-weighted area into vasogenic edema versus infiltrative tumor areas.
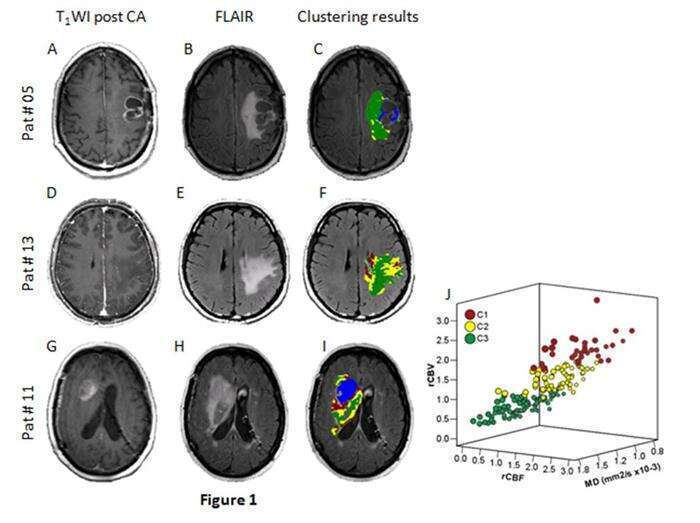
Methods. Fourteen patients with GB were longitudinally scanned, before and during bevacizumab therapy (total 40 MR scans). MRI included conventional methods, diffusion, dynamic susceptibility contrast, dynamic contrast enhancement imaging, and MR spectroscopy (MRS). Classification of the non-enhancing fluid attenuation inversion recovery (FLAIR) area was performed based on mean diffusivity, cerebral blood volume and flow maps. The components obtained were further characterized using multiple MRI parameters. Validation of classification results was obtained using MRS. Longitudinal changes of the different components were studied.
Results. The non-enhancing FLAIR lesion area was classified based on its MRI fingerprint into vasogenic edema and tumor-infiltrative area (Figure 1).
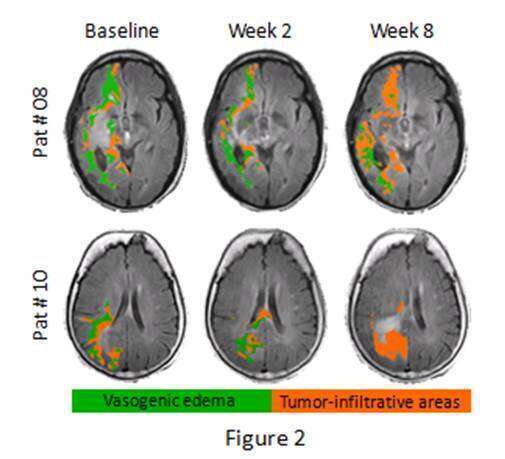
The tumor-infiltrative area demonstrated a higher malignant pattern compared to the vasogenic edema, supported by MRS. Substantial reductions of the enhanced T1 weighted and hyperintense FLAIR lesion areas were detected. However, these reductions were accompanied by a reduction of the vasogenic edema yet with an increase/ no change of the tumor-infiltrative area, in most patients (Figure 2).
Conclusions. Quantifying the infiltrative tissue in patients with GB following bevacizumab therapy provides a more accurate assessment of the response to therapy in these patients.
References: 1Groot et al. Neuro Oncol, 2010; 2Marc Med Insights Oncol, 2011;3Whitney et al. Curr Neurol Neurosci Rep, 2011; 4Zuniga et al. J Neurooncol 2010;