Background: Low cardiorespiratory fitness (CRF) is a potent risk factor for mortality. We evaluated the interaction between CRF and abdominal adiposity distribution with all-cause mortality, myocardial infarction or stroke, in patients with diabetes.
Methods:We studied 294 diabetics without coronary artery disease. CRF was quantified in metabolic equivalents by maximal treadmill testing, and categorized as low CRF (1st tertile) or high CRF (2nd and 3rd tertiles). Abdominal fat was quantified as subcutaneous (SAT) or visceral (VAT) adipose tissue from non-enhanced computed tomography scans.
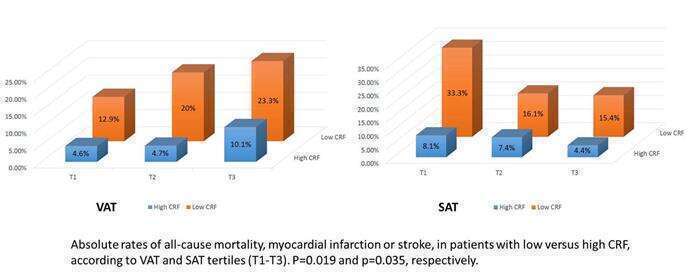
Results:There were 31 (11%) events during mean follow-up of 64 months. Low CRF was associated with adverse outcome, including after adjustment for both adiposity measures (HR 3.79, 95% CI 1.79-8.01, p<0.001). CRF level was inversely correlated with SAT but not VAT (r=-0.44, p<0.001 vs. r=-0.06, p=0.31). Absolute event rates increased progressively across VAT tertiles, but decreased across SAT tertiles. However, within each tertile, increased events were observed in the low compared to high CRF group (Figure), an association which was also observed in an adjusted multivariate proportional hazards model.
Conclusions:Although SAT and VAT differ in their association with CRF levels and absolute event rates, lower CRF is significantly associated with higher risk of mortality, myocardial infarction or stroke, regardless of abdominal adiposity pattern.