BACKGROUND:Type 2 myocardial infarction [T2MI] is myocardial necrosis secondary to oxygen supply-demand mismatch. While "plaque rupture" is the paradigm of T1MI, some systemic conditions can cause chest pain, ECG changes and biomarkers release. As heterogeneous and relatively newly defined group, data is lacking about presentation, subgroups, management and outcome of T2MI patients.
METHODS: We retrospectively reviewed medical records of patients diagnosed with T2MI in our cardiology center between years 2007-2012. After descriptive analysis, we used multivariate time depended Cox regression models to estimate the association of T2MI with the risk for 30-days and 5-years MACE [CV-death, urgent PCI, stroke and re-MI] and all-cause-mortality, and compared it to T1MI patients group matched for age, sex, diabetes, ECG changes and cardiac function.
RESULTS:The study included 107 T2MI and 107 T1MI patients. Half of T2MI developed in hospital, of those, half in medical patients and half post-surgically. Sepsis, anemia and atrial-fibrillation were the most common etiologies (incidence rate: 45%, 43% and 37%, respectively). 25% of T2-patients were managed invasively (Urgent PCI), with no difference in outcome between PCI and no-PCI groups: adjusted-Hazard-Ratio [HR] and 95% confidence-interval [CI] were 0.58 (0.16-2.14) for all-cause-mortality and 1.03 (0.29-3.65) for MACE. Angiography unmasked acute plaque rupture as the “T2MI” culprit in 29%. After multivariate analysis, T2MI was associated with significant more all-cause-mortality: HR 7.14 (1.31-38.9), P=0.023 at 30 days and 2.08 (1.14-3.81), P=0.017 at 5 years. There was no difference in CV mortality or MACE frequency.
CONCLUSIONS: In our cohort of T2MI patients, the most common triggers were sepsis, anemia and rapid atrial fibrillation. Compare to T1MI matched population: T2MI was associated with significant more all-cause-mortality, while there was no difference in CV-mortality or MACE frequency. By angiography, it was demonstrated that as much as 30% of T2MI patients may harbor acute plaque rupture and in fact suffer a mixed T1\T2MI. Even so, PCI did not show to be associated with improved outcomes.
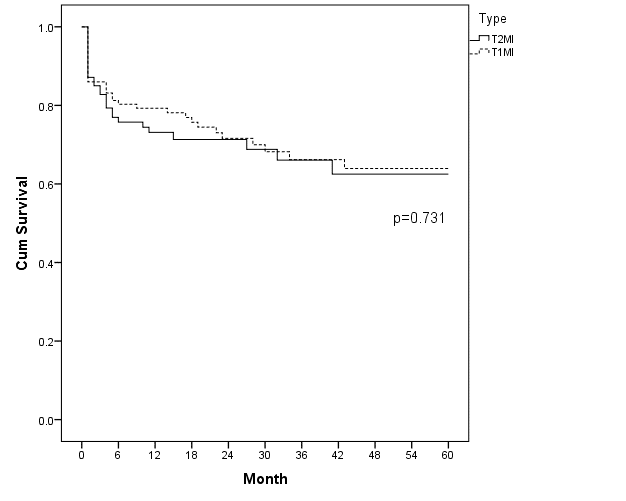
Kaplan-Meier curves for 5 years survival (A) and MACE free survival (B):
A
B