Background: Percutaneous mitral valve repair using the MitraClip technology was originally introduced to treat degenerative / myxomatous (D/M) mitral regurgitation (MR), but it is currently mostly used in patients with functional / ischemic (F/I) MR. We examined whether this therapeutic approach is justified, based on surgical risk and valve anatomy.
Methods: Consecutive patients with severe MR who were hospitalized at a tertiary care medical center were identified and their clinical records and echocardiographic studies were reviewed. Surgical risk was estimated using various risk scores, including the Society of Thoracic Surgeons (STS) risk score and EuroSCORE II. The anatomical compatibility for MitraClip invervention was assessed using the Endovascular Valve Edge-to-Edge Repair Study (EVEREST) echocardiographic criteria.
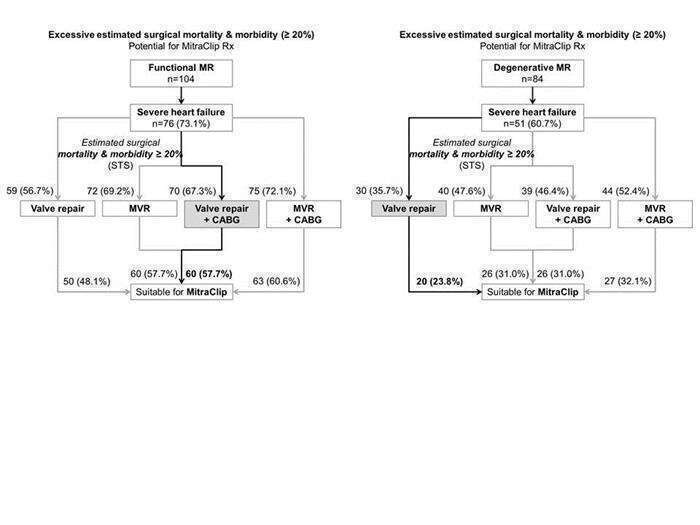
Results: Of 236 patients included in the study during 3 years, MR was F/I in 104 (44.1%), D/M in 84 (35.6%) and due to other pathologies in 48 patients (20.3%). Age and gender distribution were similar in patients with F/I (age 71±14 years, 62.5% male) and D/M MR (age 73±14 years, 66.7% male) and severe heart failure symptoms justifying intervention were evident in 73.1% and 60.7% of patients, respectively (P=0.10). Using multiple risk scores, the estimated surgical risk (mortality and major morbidity) for mitral valve repair or replacement (with or without bypass surgery) was consistently much higher in patients with F/I than D/M MR. Valve anatomy was suitable for MitraClip intervention in 87 patients (83.7%) with F/I versus only 44 patients (52.4%) with D/M MR (P<0.001). Combining the presence of severe symptoms, high surgical risk, and anatomical compatibility – significantly larger proportions of patients with F/I MR were potential candidates for MitraClip intervention than patients with D/M MR (Figures).
Conclusion: Higher surgical risk and better anatomical compatibility justify the increasing use of MitraClip intervention in patients with F/I MR, more than in patients with D/M MR.