Background: Heart failure (HF) is associated with considerable mortality. The electrocardiographic frontal QRS-T angle is a simple parameter to measure, reflects changes in the direction of the repolarization sequence and predicts outcome in patients with HF. Data regarding temporal changes in the frontal QRS-T angle in HF patients and its impact on outcome is limited.
Aim: To evaluate temporal changes in the frontal QRS-T angle and its effect on survival in patients with HF.
Methods: Baseline and follow-up QRS-T angle were calculated from the frontal QRS and T axis of the 12-lead surface electrocardiogram. Patients were followed for death.
Results: 2,929 HF patients were evaluated. Median interval between baseline ECG and follow-up ECG was 895 days, median follow-up time was 1526 days. Overall, the QRS-T angle tended to be stable, with minor changes in the angle. Median QRS-T angle change was +3°; IQR (-19° to +30°). Overall survival during follow-up was 60%. Cox regression analysis after adjustment for significant predictors including age, gender, IHD, hypertension, atrial fibrillation, body mass index, pulse, serum hemoglobin, sodium, eGFR and urea levels demonstrated that baseline and follow-up QRS-T angle were independent incremental predictors of increased mortality. A widening of the QRS-T angle during follow-up was independently associated with an increase in mortality (Figure, P<0.0001).
Conclusion: QRS-T angle is relatively stable in patient with HF and is a powerful predictor of outcome. Widening of the QRS-T angle is an ominous sign.
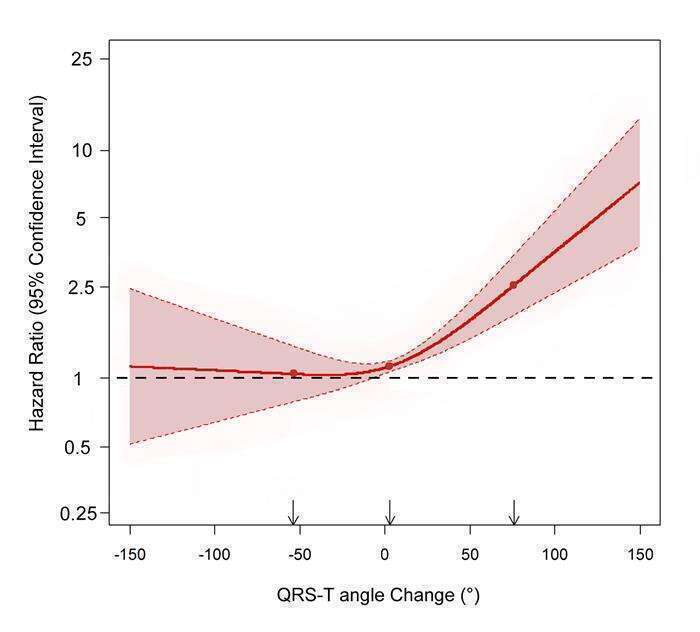
Figure: Cox regression analysis with adjusted hazard ratio for mortality (with 95% confidence interval) of the QRS-T angle change as a continuous variable using restricted cubic splines with 3 knots at the 5th, 50th and 95th percentiles of the QRS-T angle change distribution, P<0.0001.
