Background: Previous studies have shown a strong association between prompt performance of primary percutaneous coronary intervention (PCI) and reduced mortality in patients with ST-segment elevation myocardial infarction (STEMI). Accordingly, Current guidelines recommend a door-to-balloon time (D2B) of 90 minutes or less for patients undergoing primary PCI. However, results from recent contemporary cohort studies have shown inconclusive results regarding decreased door-to-balloon time and outcome.
Aim: We thought to investigate the outcome of STEMI patients according to D2B from our local STEMI registry.
Methods: We analyzed 1813 patients (age 60.3±12.2 years, 82.9% men) who underwent primary PCI within 6 hours of chest pain for STEMI at our medical center. We assessed the relation between D2B time (longer than 90 minutes or 90 minutes or less as well as in intervals of 30 minutes) and outcome (30 day, 6 month and 1 year mortality).
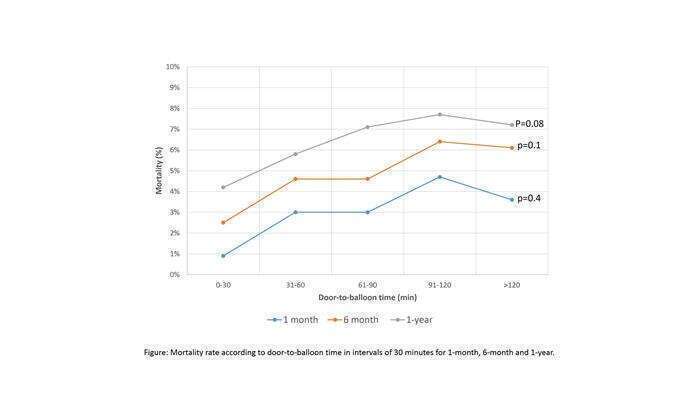
Results: Median D2B time was 60 minutes (range 0-360 minutes). During the study period a D2B time of less than 90 minutes was achieved in 76.9% of patients. Patients who underwent primary PCI in < 90 minutes had a tendency for lower early and late mortality (2.4% vs 4.1%, p=0.06 for 1-month and 5.5% vs 7.4% ,p=0.1 for 1-year). Significant reduction in 6 month mortality was observed with D2B time<90 minutes (3.9% vs 6.2%, p=0.04). The analysis of D2B time distinguished by intervals of 30 minutes [Figure 1] has demonstrated a decline in mortality <90 minutes and particularly <30 minutes for both early and late mortality outcome.
Conclusions: According to our analysis representing ‘all comers’ STEMI PCI practice, shorter D2B time was still associated with improved mortality outcome primarily when performed <30 minutes and during 6 months following the STEMI event.