Background: There are limited data regarding the relationship between age and inappropriate therapy among patients with an implantable cardioverter-defibrillator (ICD) and resynchronization therapy. We aimed to investigate this relationship and the effect of innovative ICD programming on inappropriate therapy by age groups in MADIT RIT.
Methods: In the MADIT-RIT study 1500 patients were randomized to three ICD programming arms: A) conventional with VT therapy ≥ 170; B) high-rate cut-off with VT therapy ≥ 200, and C) prolonged 60 sec delay for VT therapy ≥ 170.
The relationship between age, the risk of a first inappropriate ICD therapy (including antitachycardia pacing [ATP] or shock) and ICD programming was assessed among patients enrolled in the MADIT-RIT.
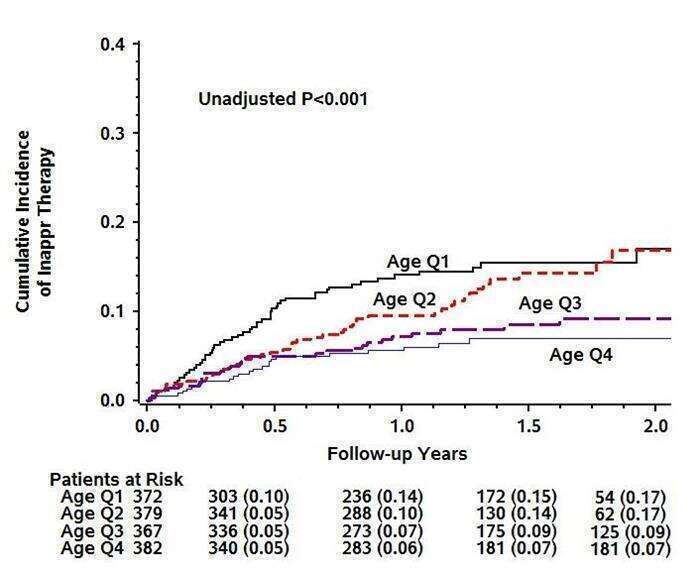
Results: Cumulative incidence function graphs showed an inverse relationship between increasing quartiles of age (Q1: ≤55, Q2: 56-64, Q3: 65-71, and Q4: ≥72 years) and the risk for inappropriate therapy. (Figure)
Multivariate analysis showed that each increasing decade of life was independently associated with 34% (p <0.001), 27% (p <0.001), and 26% (p<0.001) reduced risk for inappropriate shock, inappropriate ATP, and any inappropriate therapy, respectively. These trends were evident in the 3 randomized programming arms. Furthermore, innovative ICD programming, in arms B and C as compared with arm A, was associated with a significant reduction in the risk of inappropriate therapies across all age quartiles (p<0.001 for all).
Conclusions: Among patients with a primary prevention indication for an ICD, there is an inverse relationship between age and inappropriate ICD therapy. Innovative ICD programming of high-rate cut-off or prolonged delay for VT therapy is associated with significant reductions in inappropriate therapy among all age groups.