Introduction: There is limited data regarding eGFR and CRT response. We sought to evaluate the impact of baseline eGFR on long term mortality in CRT patients.
Methods: The study included 171 patients implanted with CRT device from 2007 to 2010, alive at one year post-implant. Patients had clinical and echocardiographic assessment in the first year after CRT. Clinical response was defined by a composite score based on NYHA class, 6-minute walk test and Quality of Life. Patients with normal renal function (eGFR ³ 60 ml/min/1.73m2) were compared to those with renal dysfunction (eGFR < 60 ml/min/1.73m2). Survival data were obtained up to 6 years post-implant.
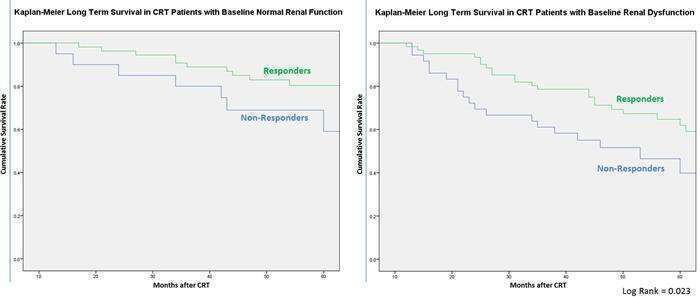
Results: During the follow-up period of 4.2±1.4 years 68 patients died. Patients with renal dysfunction were older (72.2 ± 8.1 years vs 64.4 ± 12.1 years; p=0.001) and had higher prevalence of ischemic heart disease (74% vs 57%; p=0.013). The 4-year mortality was significantly higher in the renal dysfunction group (51.5% vs 24.3%; Log Rank = 0.026). Although responders had higher 4-year mortality rates in the presence of renal dysfunction (49.2% vs 20.4%), they still benefit from CRT compared to non-responders (survival 50.8% vs 44.4%). Multivariate analysis demonstrated that clinical response to CRT at one year was associated with 50% reduction in the 4-year all-cause mortality (HR 0.512; p=0.007) after adjustment for renal function (HR 1.781; p=0.005).
Conclusions: Clinical response at one year is associated with long-term CRT survival benefit in patients with baseline renal dysfunction, despite worse overall prognosis.