Background: Lipoprotein associated Phospholipase A2 (Lp-PLA2) is a specific biomarker of vascular inflammation and atherosclerosis. Lp-PLA2 levels were reported to be associated with coronary heart disease (CHD) and mortality. In contrary, data on the association between Lp-PLA2 activity and prognosis among CHD patients are scarce.
Method: Among 3122 CHD patients included in the Bezafibrate Infraction Prevention (BIP) study, 2538 survived to the 5th follow-up year and had available frozen blood samples. Lp-PLA2 activity was measured with calorimetric activity method.
Results: patients in the 3rd activity tertile (≥ 247.21 nmol/ml/min) were on average, a year younger, two centimeters taller, had lower systolic blood pressure, with higher prevalence of: men, metabolic syndrome, coronary artery bypass graft and smoking compared to 1st tertile (≤ 202.00) patients (p trend≤0.01 for all). Patients in the 3rd tertile had also higher total and low density lipoprotein cholesterol (LDL-C), non-high density lipoprotein cholesterol (nonHDL-C), triglyceride and fibrinogen and lower HDL-C levels. Lp-PLA2 correlated with age (R=-0.065), HDL-C (-0.435), LDL-C (0.344), nonHDL-C (0.373), fibrinogen (0.142) or hemoglobin (0.239)
but not with C-reactive protein.
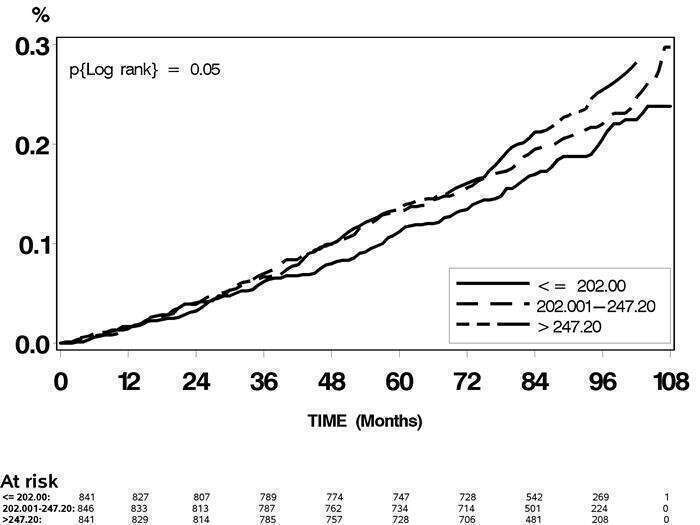
Over 8.3 follow-up years (209,158 person-months), 554 patients died. Patients in the 3rd activity tertile had higher cumulative mortality probability compared to the 1st or 2nd (202.01-247.20) tertiles (Figure). The age and sex adjusted mortality hazard ratio (HR) associated with the 3rd tertile was 1.35 compared to the 1st tertile (95% confidence interval: 1.10-1.66). HR did not significantly change upon further adjustment for: diabetes mellitus, hypertension, body mass index, CHD family history, smoking, education and ethnicity. However, inclusion of Lp-PLA2 activity in the model did not improve its discrimination ability beyond other risk factors (C index=0.685 vs 0.683 with and without activity, respectively).
Conclusion: Lp-PLA2 activity is a marker of mortality among chronic CHD patients but does not improve prediction beyond other risk factors.