Background: Transcatheter aortic-valve implantation (TAVI) has been associated with 2-5% risk of peri-procedural stroke. Several mechanisms were proposed for the stroke risk including a pro-thrombotic state and embolization of calcified material from the aortic valve. Accordingly, it is common to administer dual anti-platelet treatment (DAPT) for 3-6 months following TAVI. The biologic response to aspirin and clopidogrel is heterogeneous, and low response, known as high on treatment platelet reactivity (HTPR) may be associated with adverse thrombotic events, including stroke. The prevalence of HTPR in patients undergoing TAVI has not been yet reported. Therefore, we aimed to assess the variability in response and rates of HTPR in patients undergoing TAVI.
Methods: We examined platelet reactivity and response to clopidogrel and aspirin using the VerifyNow P2Y12 assay and the multiple electrode aggregometry assay (Multiplate analyzer) in response to ADP and arachidonic acid in patients who underwent TAVI at 3 different time points: baseline, 1-2 days following the procedure and 30 day follow up.
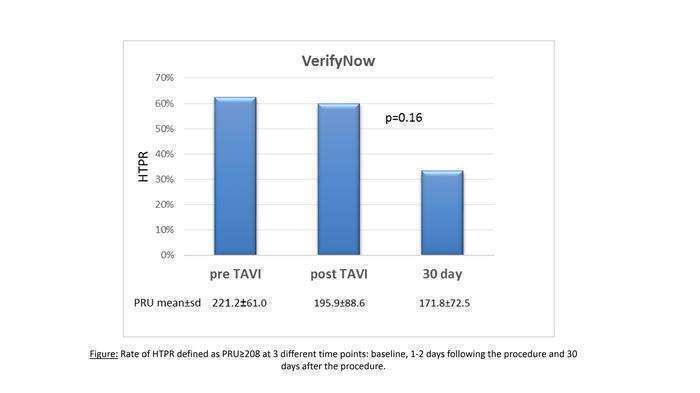
Results: Our preliminary results include 22 consecutive high risk patients with severe aortic stenosis (mean age 81±5.7, 68.2% women) who underwent successful TAVI. Prior to the procedure 15 (68.2%) patients were chronically treated with aspirin and 8 (36.4%) with clopidogrel. HTPR rates for both aspirin and clopidogrel were high prior to TAVI and early after the procedure, but improved significantly 30 days after TAVI (Figure). According to the multiplate analyzer, HTPR rates for aspirin were 20% at baseline, 12% 1 to 2 days after the procedure and none at 30 days (P=0.4).
Conclusions: Patients undergoing TAVI for severe aortic stenosis and treated with DAPT have high rates of HTPR during the peri-procedural period, which subside profoundly after 1 month. These novel findings should be confirmed and expanded but may have clinical implications for the anti-platelet management of these patients.