Background: Two-dimensional strain (2DS) based on echocardiographic speckle-tracking may aid in diagnosing segmental left ventricular (LV) dysfunction, but the accuracy of this technique has not been adequately established in clinical practice.
Methods: Echocardiography was prospectively performed in 30 patients (pts) with ST-elevation myocardial infarction (MI) following successful primary coronary intervention (age 56±10 years; 22 men; infarct-related coronary artery [IRA] – left anterior descending: 12 pts; circumflex: 7 pts, right: 11 pts; LV ejection fraction: 49±8%, range: 30-65%). Only pts with a first MI and single-vessel coronary artery disease were included in the study. Peak longitudinal systolic strain (pLS), at or before aortic valve closure, was measured by 2-DS in 3 apical views (EchoPAC, GE) and compared to eyeball assessment of segmental function by experienced echocardiographers.
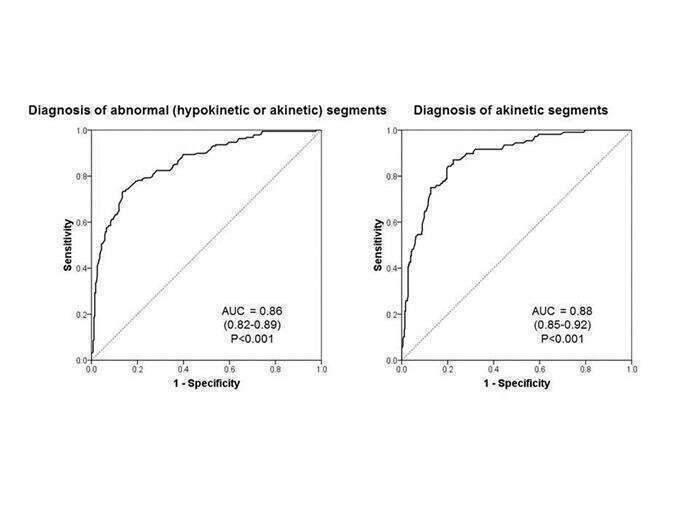
Results: Of 480 LV segments, pLS was measurable in 464 segments (96.7% feasibility). Eighty segments were hypokinetic (17.2%) and 108 (23.3%) were akinetic by visual assessment. Segmental dysfunction matched the IRA in all pts. pLS differed markedly between normal (-18.3±5.3%), hypokinetic (-12.8±5.7%) and akinetic segments (-6.8±7.0%) (P<0.001). Using receiver operating characteristics (ROC) analysis, the area under the curve (AUC) for detecting any segmental dysfunction (hypokinetic or akinetic segments) by pLS was 0.86 (95% confidence interval 0.82-0.89; P<0.001) and for detecting akinetic segments was 0.88 (0.85-0.92; P<0.001) (Figures). An absolute value of pLS <15.2% (lowest quartile of pLS in normal segments) had a sensitivity, specificity, positive and negative predictive values of 79.3%, 76.5%, 69.6%, and 84.4% in diagnosing any segmental abnormality (hypokinetic or akinetic segments). An absolute pLS <10.8% (highest quartile of pLS in akinetic segments) had diagnostic values of 75.0%, 87.4%, 64.3%, and 92.0%, respectively, for akinetic segments.
Conclusion: 2DS may aid in the diagnosis of segmental LV dysfunction. However, the overall diagnostic accuracy of pLS is sub-optimal and additional 2DS parameters need to be examined.