Background: Significant chronic kidney disease is associated with increased cardiovascular morbidity (CM). However, there are sparse data regarding the association of changes in kidney function in the normal or mildly impaired range and CM.
Aim: To examine the association between kidney function within the normal or mildly impaired range and incident CM in a large, population-based cohort with no prior CM.
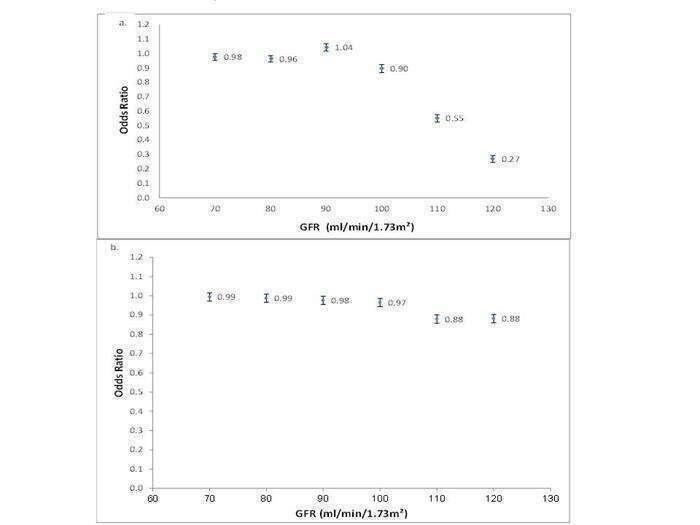
Methods: A pilot, retrospective, population-based analysis derived from the Clalit Health System database. Glomerular filtration rate (GFR) was measured using Chronic Kidney Disease EPIdemiology collaboration (CKD-EPI) and the Modification of Diet in Renal Disease (MDRD) formulas. For each formula, we analyzed only patients with 60< GFR< 130 ml/min/1.73m2 and no prior CM.
Results: The mean age of our cohort was 49.0± 17.0 years, with a male/female ratio of 0.7 and a mean GFR of 90.9± 17.3 ml/min/1.73m
2. During a median follow up of 96.0 months and >10 million patient-years of follow-up, a total of 103,506 and 104,315 events were recorded (Incident CM rate of 4.4% and 4.6% using CKD-EPI and MDRD formulas, respectively). Using multivariable analysis adjusted for age, gender and cardiovascular risk factors, we found than an increase of 10 units in GFR was independently associated with a decrease of 2.3% and 0.9% in incident CM (using CKD-EPI and MDRD, respectively, p<0.001 for both).
Conclusion: Our findings, derived from a large, population-based cohort, demonstrate that an increase in GFR, even within the normal or mildly impaired range, is independently associated with reduced incident CM in the general population with no prior CM. Thus, kidney function may be used as a risk marker for incident CM among patients with and without significant chronic kidney disease.