Background: Transradial coronary catheterization (TRCC) reduces the risk of vascular access-site bleeding compared to the transfemoral approach and is preferred by patients, however it may result in radial artery occlusion (RAO). Large-bore 7F sheaths enable complex coronary interventions, however increased sheath size may increase the likelihood of subsequent RAO. We studied long-term radial artery patency in a cohort of patients who had undergone TRCC with a 7F sheath.
Methods: Patients who had undergone 7F TRCC were identified from our prospective catheterization laboratory database. Radial artery patency was assessed by ultrasound Doppler analysis of antegrade radial blood flow and by the Barbeau test, with assessment of palmar perfusion by digital pulse oxymetry while occluding the ulnar artery. The study was approved by the IRB.
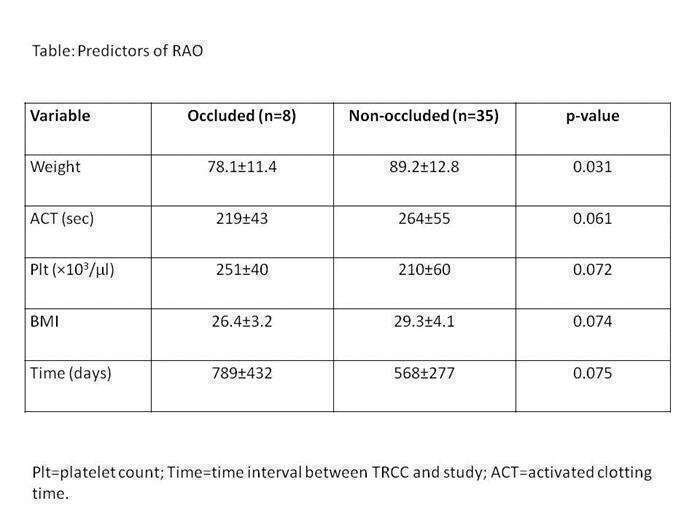
Results: Forty-three patients who had undergone 7F TRCC were studied. In all patients dual palmar blood supply had been confirmed prior to TRCC. Mean age was 65±10 years. A 7F sheath was used for facilitated thrombus aspiration in 26 (60%) patients with STEMI and for facilitating complex bifurcation stenting in the remainder. Coronary stenting was performed in 32 (74.5%). All patients received intra-arterial verapamil and intra-venous unfractionated heparin and mean activated clotting time (ACT) was 247±56 seconds. Twenty-four (56%) patients received a glycoprotein IIbIIIa inhibitor. No vascular site complications occurred following the procedure. Mean time interval from TRCC to inclusion in the study was 507±317 days. The radial artery was patent in 35 (81%). All 8 (19 %) RAO cases were asymptomatic. Reduced body weight was the only significant predictor of RAO (78.1±11.4 vs. 89.2± 12.8 kg, p=0.031).
Conclusions: Asymptomatic RAO was found in approximately 1 in 5 patients undergoing 7F TRCC and was associated with lower body weight. Our findings suggest that need for large-bore 7F access does not necessarily preclude the option of transradial access.