Background: Ischemic time is an important prognostic factor in STEMI patients. Emergency medical service (EMS) utilization can reduce different components of ischemic time by appropriate triage of STEMI patients.
Methods: Data from the Acute Coronary Survey in Israel registry (ACSIS) 2000-2010 were analyzed to evaluate factors associated with EMS use, and its impact on different components of ischemic time.
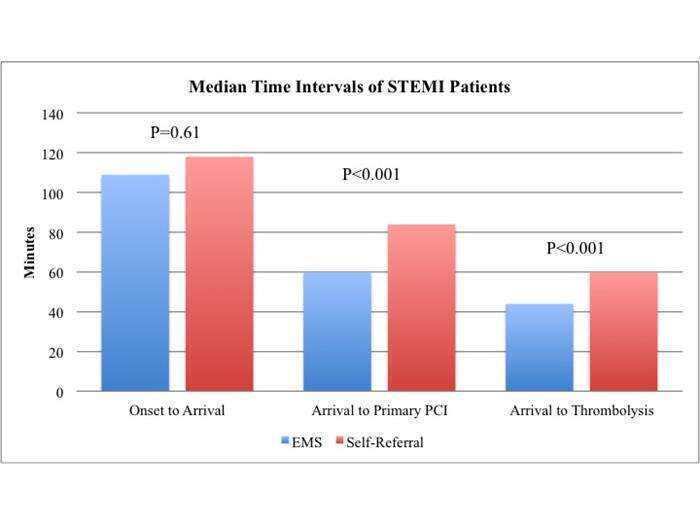
Results: The study population comprised of 3031 STEMI patients treated with primary reperfusion therapy (64% primary PCI and 36% thrombolysis) among whom only 1566 patients (52%) used EMS. Predictors of EMS use were family history of ischemic heart disease (OR=1.25, p=0.02), syncope (OR=1.37, p=0.04) and dyspnea (OR=2.02, p=0.006), while hypertension and smoking were predictors of self referral (OR=1.22, p=0.02 and OR=1.27, p=0.005, respectively). EMS use reduced onset-to-reperfusion time (175 vs. 195 min. p<0.001), mainly by reducing arrival-to-reperfusion time, either in patients treated with primary PCI (60 vs. 86 min. p<0.001) or thrombolysis (44 vs. 60 min. p<0.001). On a multi-variate analysis, reduction in arrival-to-reperfusion time was associated with reduced
cardiovascular events at 30 days (OR=0.51, p=0.02).
Conclusion: High-risk STEMI patients, with a presentation of heart failure and syncope are more likely to use EMS which reduces ischemic time intervals, which are associated with reduced cardiovascular events at 30 days.