Background: Chronic total occlusion (CTO) is one of the most technically challenging lesions for percutaneous coronary intervention (PCI). Only a small part of CTOs are intervened, perhaps because procedural success is limited by difficulties crossing and/or dilating the occluded segment. Improved techniques and the introduction of newer dedicated devices [wires, micro-catheters] have improved the success rate in crossing and treating CTO lesions.
Aims: We hypothesized that by using new tools and techniques, the known predictors of failure of CTO recanalization [heavy calcification, blunt/ non-taperd occlusion, bridging collaterals] become less significant. We thus aimed to analyze the effects of these predictors on success of recanalization.
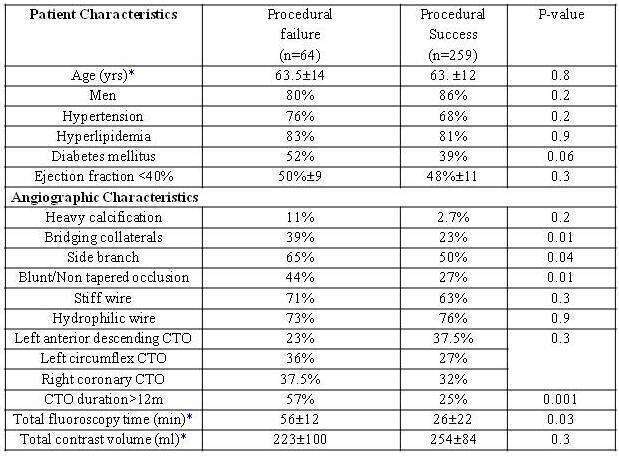
Methods: We analyzed a total of 323 consecutive patients in whom CTO recanalization was attempted. We compared patient and angiographic characteristics between successful recanalization group (259 patients) and failed recanalization group (64 patients). CTO was defined as occlusion duration of > 3 months or of unknown duration. Successful recanalization was defined as crossing a CTO lesion.
Results: Procedural success was observed in 80% of attempts.
Patients in whom recanalization had failed tended to have diabetes (52% vs. 39%,p=0.06), had bridging collaterals (39% vs. 23%, p=0.01), a side branch was involved (65% vs. 50%,p=0.04)and had blunt/Non tapered occlusion (44% vs. 27%,p=0.01).
Conclusions: Despite the use of dedicated wires, and new techniques for revascularization, the old predictors of failure of recanalization still played a role.