Mitral Regurgitation (MR) is generally assessed by EchoDoppler, using multiple parameters which are mostly qualitative in nature. The PISA (Proximal Isovelocity Surface Area) method is used for quantitative evaluation however it is based on simplistic assumptions, including hemispheric geometry, and uniform orifice area through systole. Cardiac magnetic resonance (CMR) enables detailed 3D evaluation of flow vectors making it theoretically suitable for accurate quantification of MR without any assumptions.
Aim: To test the feasibility of performing a quantitative estimation of MR regurgitant volume (RVol) by the PISA approach, using CMR 3D velocity vectors, compared to Doppler and CMR volume-based RVol.
Methods: In a prospectively designed study, 19 patients with various grades of MR underwent CMR and EchoDoppler on the same day. By CMR, multiple slices were obtained parallel to the mitral valve by phase-contrast imaging, as well as standard cine images through the ventricles for left and right ventricular volume measurements. The area of proximal flow convergence was identified and, using dedicated software, the perimeter was automatically measured for each temporal phase. The 3DRVol was calculated as the sum of PISA perimeters throughout systole, multiplied by slice width. CMR Volume-based RVol was calculated as the difference between left and right ventricular stroke volumes.
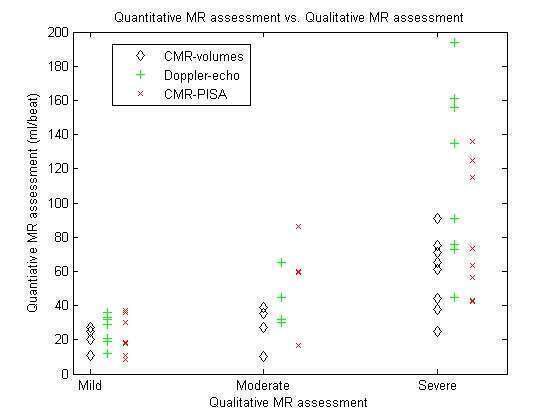
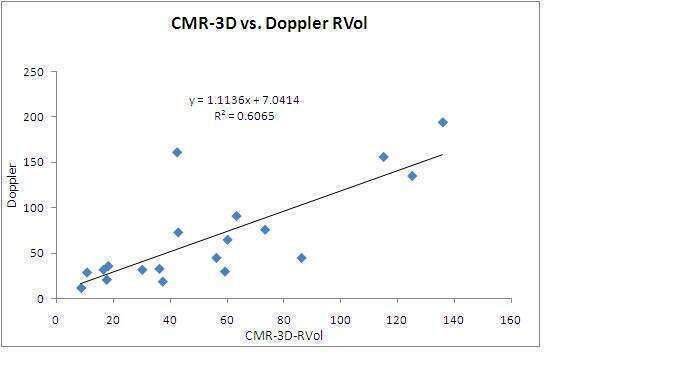
Results: For mild, moderate and severe MR, 3DRVol was 20±11ml, 52±26ml and 82±38ml compared to Doppler-RVol 27±9ml, 38±18ml and 116±52ml. CMR 3DRVol correlated well with Doppler-RVol (r=0.78, figure) and with Volume-based RVol (r=0.77). On average 3DRVol was 13ml less than Doppler-RVol, but 18ml larger than CMR-volume-based RVol (figure). The observed 3D shape of the PISA envelope by 3D CMR was closer to a hemiellipsoid than a hemisphere.
Conclusion: This feasibility study suggests that CMR-based 3D-PISA may be able to assess MR severity quantitatively without any geometric assumptions however further validation is required.