A four year old boy newly diagnosed with diabetes mellitus type one was admitted to the Department of Pediatrics. In the last four weeks the boy was complaining increasing fatigue, loss of appetite, polydipsia, nocturia and body weight loss of 4 kg.
At admission the patient was in confusional state presenting apathy and drowsiness. On physical examination severe dehydration was noted with tachycardia 110-120/min, weak pulse, tachypnoe. The laboratory exams revealed severe hyperglycemia of 595mg/dl and a number of markers of ketoacidosis and dehydration: pH 7.18 BE–22, HCO3- 5.0 mmol/l; Na 147 mEq/l; K 6.1 mEq/l; hematocrit 35.9 %; RBC 4.26 T/l, PLT 325 G/l; WBC 10.2 G/l; creatinine 1.4 mg/dl; osmolarity -330 mOsm/kg H20; CRP-0,2 mg/l.
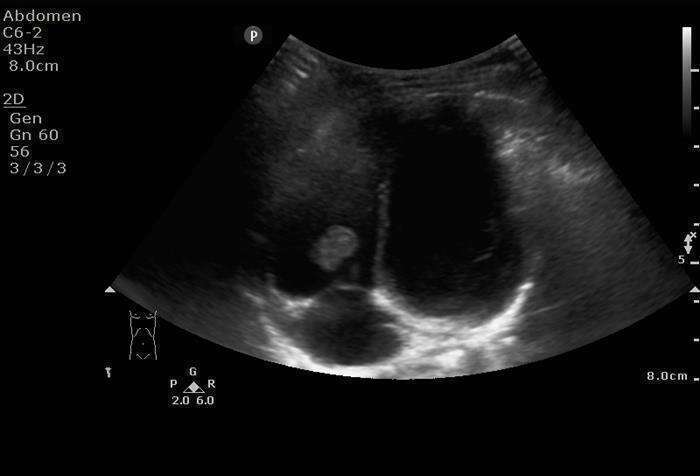
As emergency treatment the patient received insulin and fluids intravenously for 22 hours; afterwards the insulin was administered subcutaneously. At day 6 of hospitalization bedside abdomen and heart ultrasound imaging with convex probe was performed. A pathological lesion in the right ventricle was noted (Fig.1); hence immediately further detailed echocardiography examination was performed. The finding proved to be a movable, well-confined, isoechogenic solid lesion attached to the right ventricle chordate in the subvalvular tricuspid valve (TV) apparatus sized 13.9 8.4 mm. Besides, moderate TV insufficiency was noted.
Differential diagnosis included thrombus, vegetation or a heart tumor. Additional tests consisted of blood cultures (bacterial and fungal), coagulation tests (including protein C and S levels, activated protein C resistance, plasminogen and antithrombin III serum levels), homocysteine and complement C3a and C4 levels – all within the range of norm.
The patient was eventually qualified for surgical removal of the lesion from the right ventricle. On histopathological examination the removed intraventricular heart tumor was diagnosed to be a thrombus with a predominantly neutrophil infiltration.
Currently, 18 months later, the patient is in very good general condition. Echocardiography performed every 3 months revealed no distant complications. The TV insufficiency is of moderate grade showing no progression over time.
To our knowledge this is the first report of thrombus in the right ventricle in a child with severe ketoacidosis.