Prior studies demonstrated the effectiveness of extracorporeal shockwave therapy (ESWT) in osteonecrosis of femoral head (ONFH), and the results were superior to core decompression and bone graft. Other study showed that ESWT produced focal regeneration and systemic manifestation. In those studies, 6000 impulses of ESWT at 28 KV (equivalent to 0.474 mJ/mm²) were applied to the affected femoral head. However, the ESWT dosages were based on clinical experience and manufacturer recommendations, and the optimal dosage had not been scientifically validated. To our best knowledge, there has been no study reporting the optimal dosage of ESWT in ONFH. The purpose of this study was to analyze the effect of dosage escalation on angiogenesis promotion after ESWT in ONFH.
Thirty-three patients with 42 hips were divided into three groups. Group A consisted of 10 patients with 16 hips that received 2000 impulses of ESWT at 24 Kv (low dosage). Group B consisted of 11 with 14 hips that received 4000 impulses of ESWT at 24 Kv (medium dosage). Group C consisted of 12 patients with 12 hips that received 6000 impulses of ESWT at 24 Kv (high dosage). The evaluation parameters included clinical assessment, radiograph and microcirculatory dynamic contrast enhancement MRI. In addition, ten milliliters of peripheral blood were obtained for the measurements of serum NO3 and VEGF for angiogenesis, BMP-2 and osteocalcin for osteogenesis, TGF-α and IL-6 and sICAM1 for inflammation, substance p and calcitonin-gene related peptide for pain perception, and DKK-1 and insulin-like growth factor for tissue regeneration bio-markers before treatment and at 1, 3, 6 and 12 months after treatment.
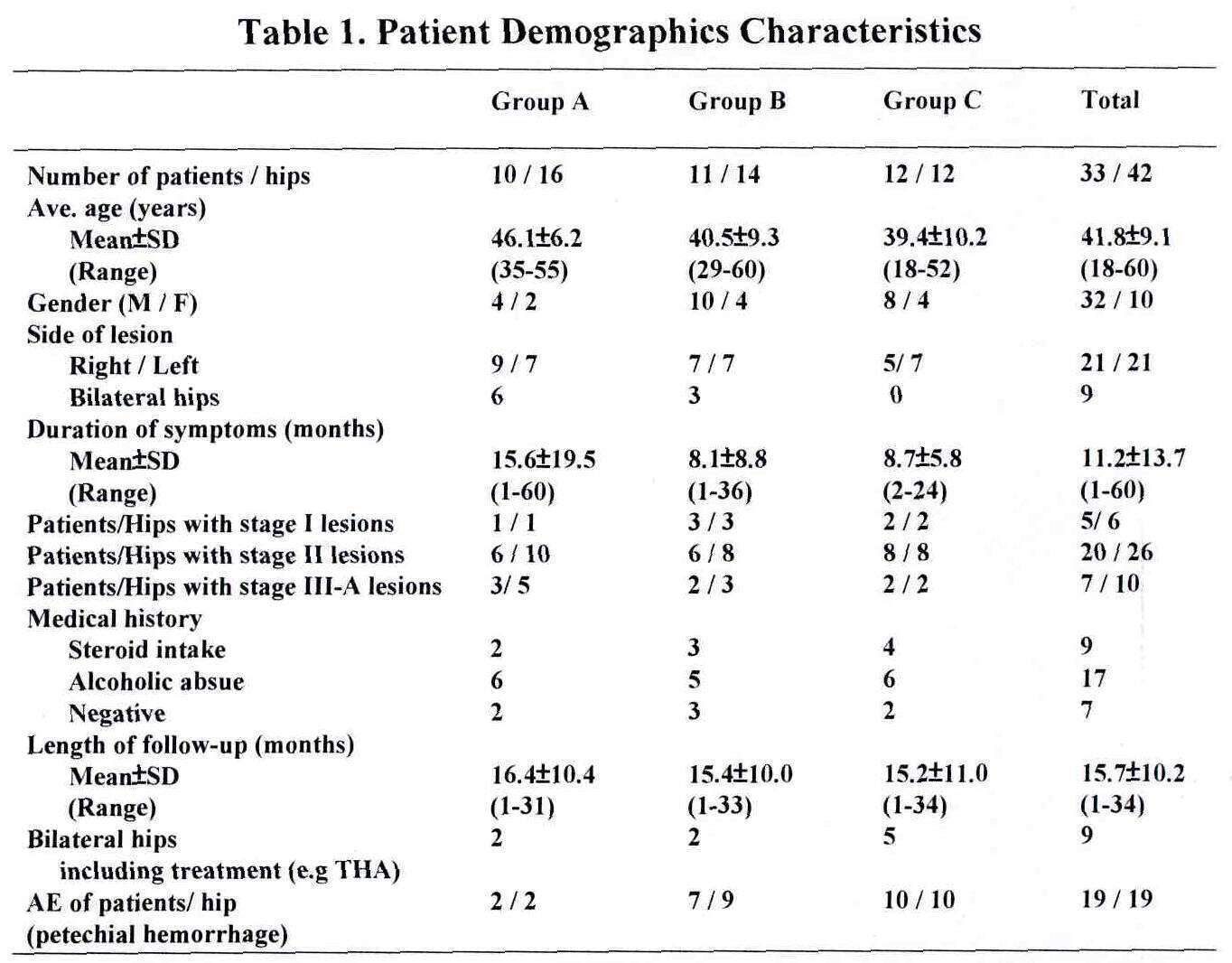
The patient demographic characteristics are summarized in Table 1. There are no significant differences in age, gender, duration and severity of disease among three groups.
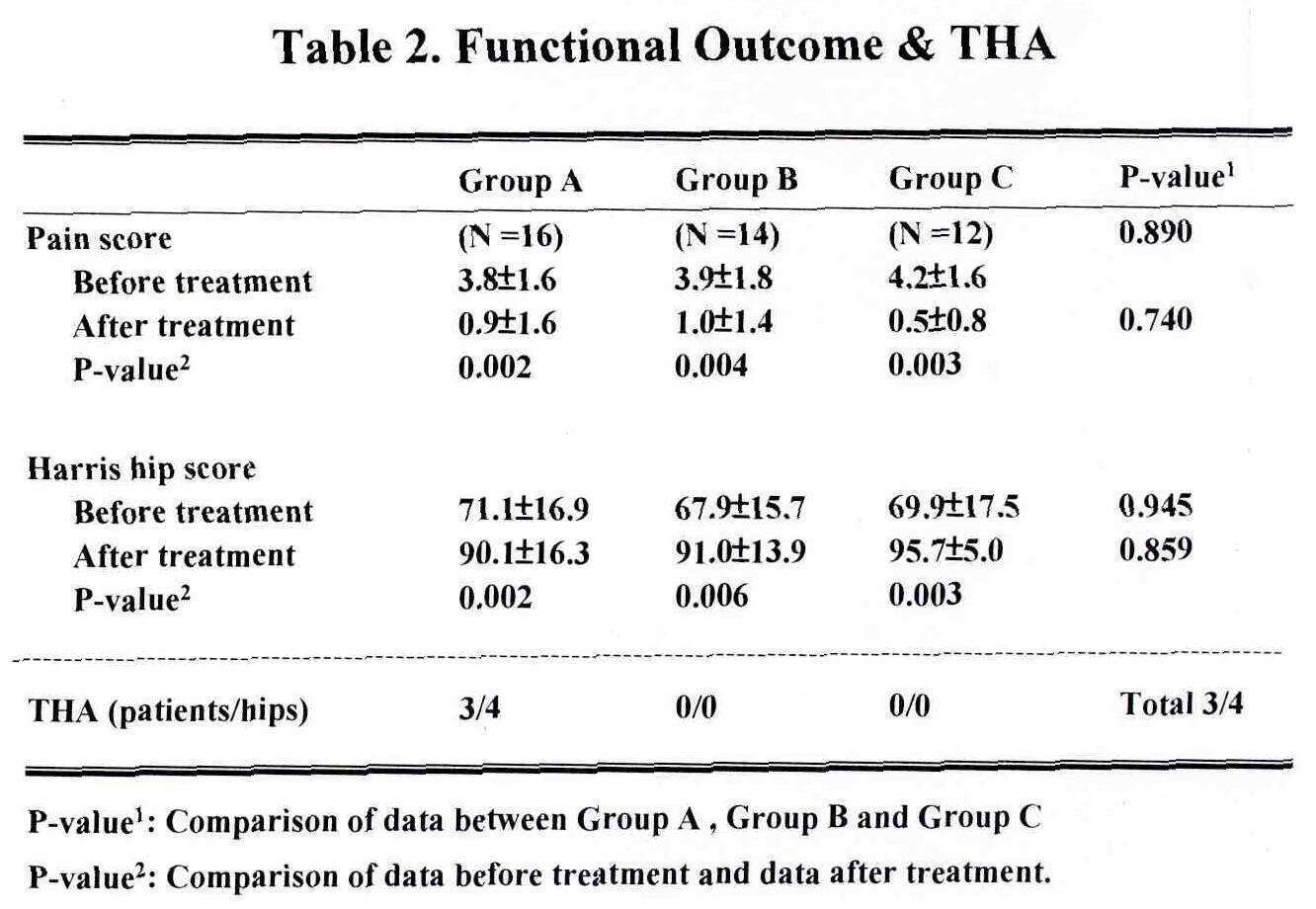
The functional outcomes and the numbers of total hip replacement are summarized in Table 2. Significant improvements in pain and Harris hip scores were observed after treatment in all three groups (P<0.05), however, the differences among the three groups were statistically not significant (P>0.05). Three patients with 4 hips in Group A underwent total hip replacement (THA) during the course of treatment because of increasing pain. No THA was performed in Group B and Group C.
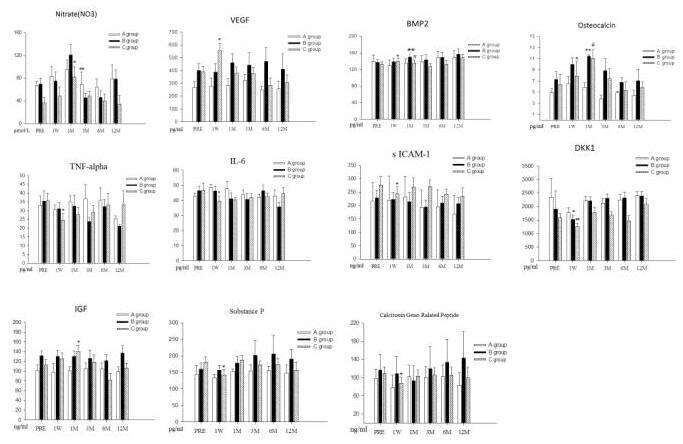
Serum NO3, VEGF, BMP2, Osteocalcin, TNF-α, Il-6, sICAM1, DKK-1, IGF, Substance P and CGRP are showed in Figure.
Serum NO3 and VEGF: Group C showed significant increase of VEGF in one week after ESWT (P=0.011) as compared to Group A and Group B. Groups B and C showed more pronounced increases of NO3, and significant elevations were observed in 1 month after ESWT (P=0.004, 0.002).
Serum BMP-2 and osteocalcin: Group B and Group C showed more pronounced increases in BMP-2 and osteocalcin, and significant elevations were observed in one week to one month after ESWT (P=0.034, 0.013).
Serum TNF-α, IL-6 and sICAM1: Group C showed significant reduction in serum TNF-α, IL-6 and sICAM1 in one week after ESWT as compared to Group B and Group C (P=0.011,0.041,0.005).
Serum DKK-1 and IGF: Group B and Group C showed significant increases in DKK-1 in one week (P=0.021,0.005),and Group C showed significant increase in IGF in one month (P=0.010) after ESWT respectively.
Serum substance P and calcitonin-gene related peptide (CGRP): Group C showed significant reduction in substance P and CGRP in one week after ESWT as compared to Group B and Group C (P=0.004).
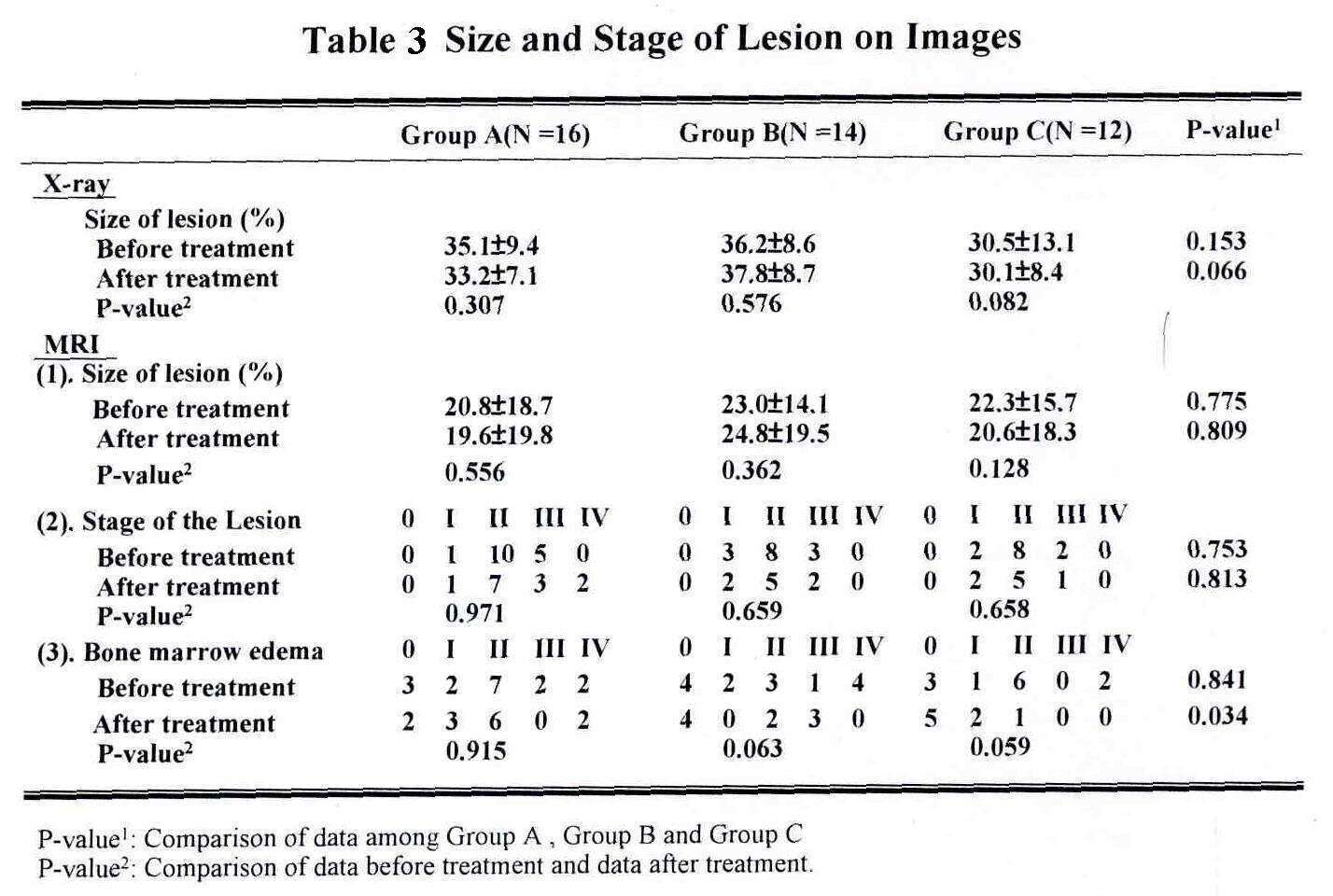
The size and the stage of the lesion on X-rays and MRI are summarized in Table 3. No significant differences in size and stage of the lesion were noticed before and after treatment within the same group (P>0.05) and among the three groups (P>0.05). Bone marrow edema on MRI significantly reduced after ESWT, and the differences among the three groups were statistically significant favoring the high dosage Group C (P=0.034).
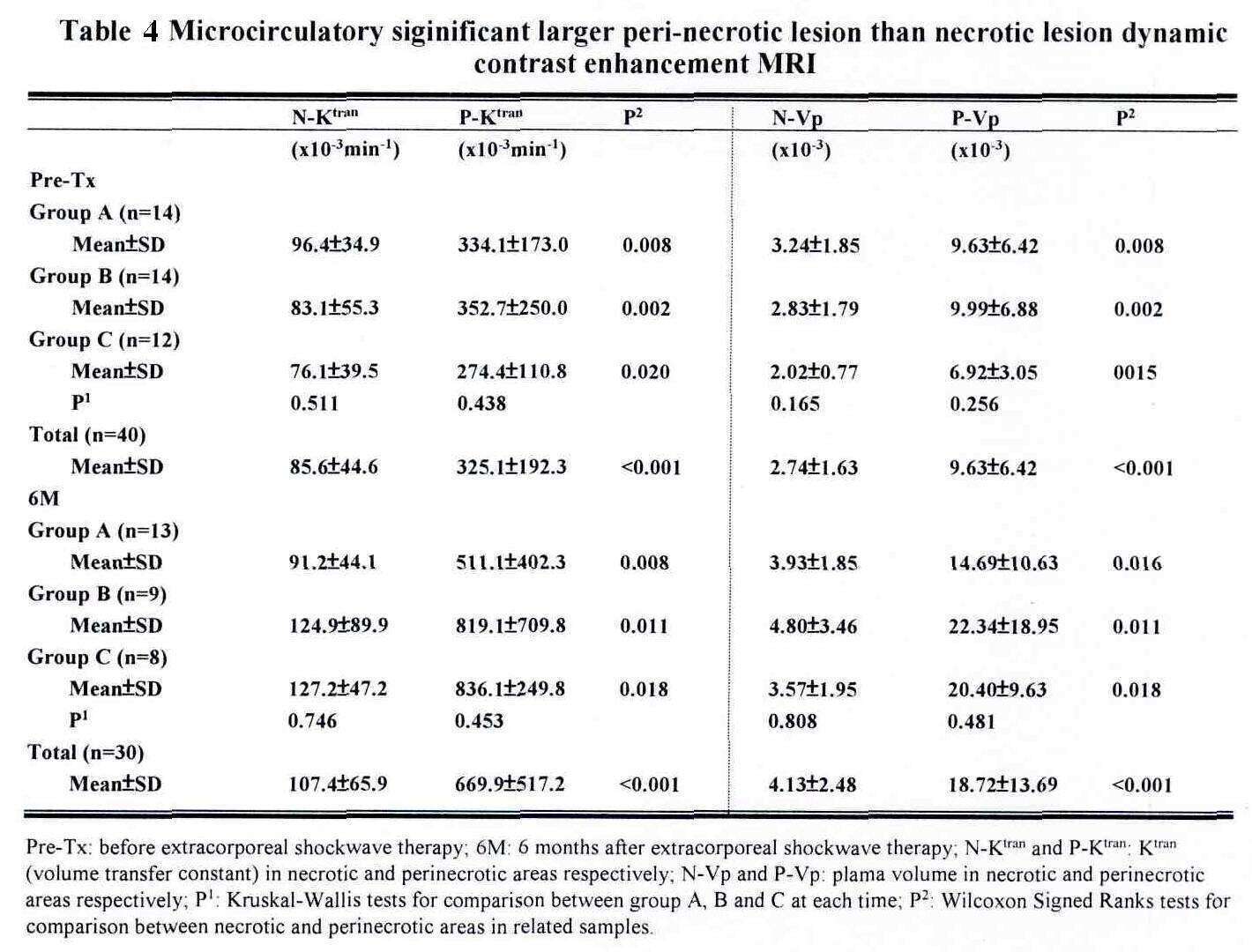
Microcirculatory dynamic contrast enhancement MRI before and 6 months after ESWT are summarized in Table 4. There were no significant differences of Ktran (volume transfer constant or endothelial permeability or surface area of microcirculation in bone) and Vp (plasma volume) in necrotic and peri-necrotic areas among the three groups at pre-treatment and 6 months (all P>0.05). All Ktran and VP in the peri-necrotic areas of the femoral head were significantly greater than those in the necrotic areas of the femoral head at pre-treatment and 6 months (all P<0.05).
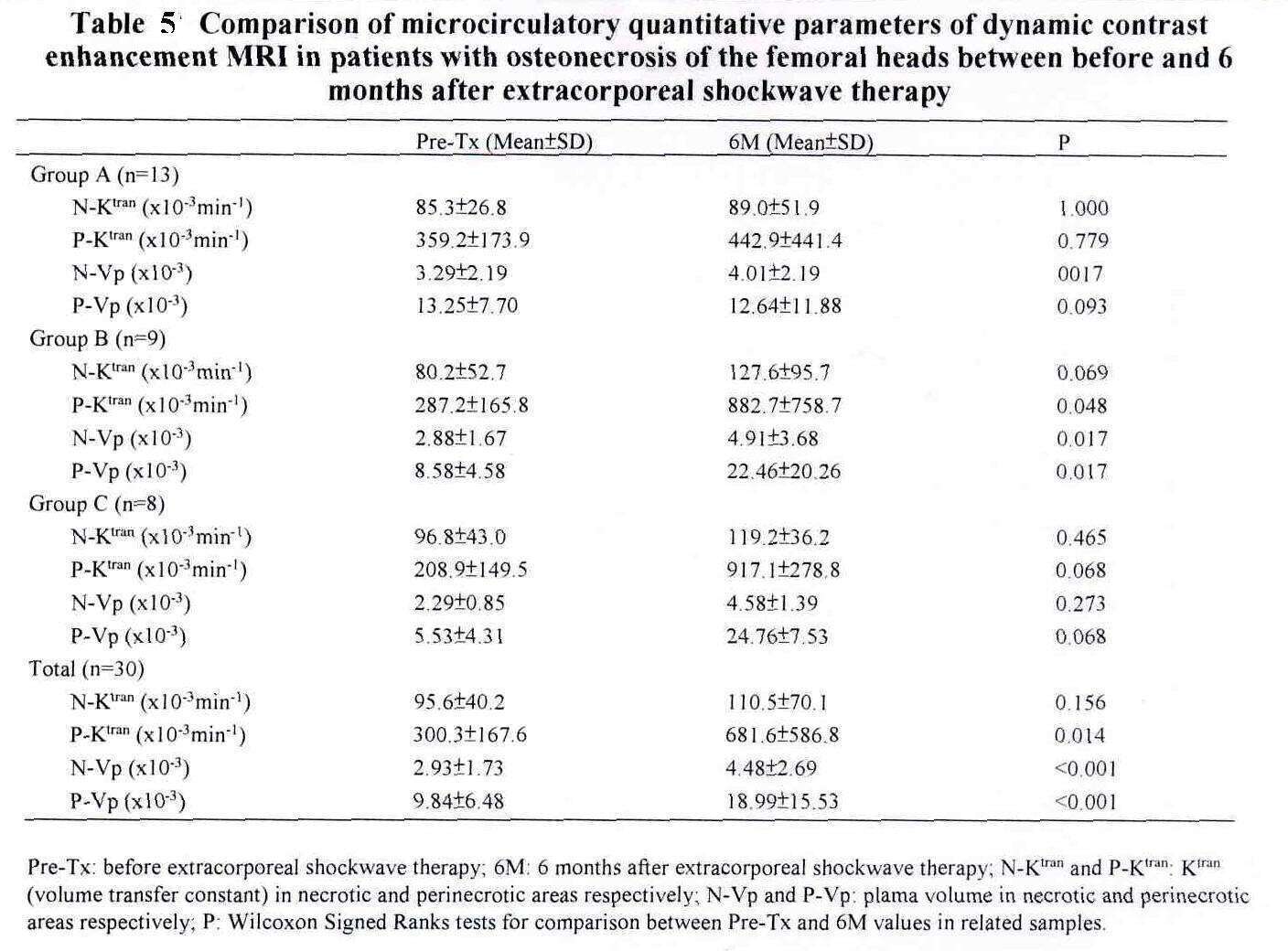
Comparison of microcirculatory dynamic contrast enhancement MRI before treatment and at 6 months after ESWT are summarized in Table 5. In patients with ONFH, our study demonstrated the Ktran and Vp in the peri-necrotic areas were significantly greater than those in the necrotic areas at the pre-treatment and 6 months. Reactive changes with increased vascularity in the peri-necrotic areas might lead to greater Ktran and Vp. No significant differences of Ktran and Vp in the necrotic and peri-necrotic areas among the three groups at 6 months after ESWT were noted in this study. Therefore, increased dosage of ESWT did not significantly change the permeability and microcirculation in the treatment site. We also demonstrated that Ktran in the peri-necrotic area and Vp in the necrotic and peri-necrotic areas at 6 months were significantly greater than those at pre-treatment in all cases. These findings correlated with the angiogenesis promoting therapeutic effect of ESWT. The mixed results of Ktran and Vp in the necrotic and peri-necrotic areas 6 months after ESWT may be attributed to limited case numbers.
In conclusion, high dosage ESWT is more effective than low dosage ESWT for ONFH. High dosage ESWT demonstrated significantly more pronounced angiogenesis promoting therapeutic effects. However, increased ESWT dosage did not significantly change the permeability and microcirculation in the treatment site. Additional studies are needed to further correlate the intimate relationship between angiogenesis promoting effect and increased permeability of the femoral head after ESWT in ONFH.
