Introduction: Response to Cardiac Resynchronization Therapy (CRT) is known to be affected by the pacing site strain properties. Local strain measurement is possible with Speckle Tracking Echocardiography and Cardiac Magnetic Resonance imaging. Yet, neither is routinely available. CardNav is a novel system measuring epicardial strain by tracking bifurcations and curvatures in venograms using computer vision. The prognostic value of strain amplitude measured angiographically at the Left Ventricular (LV) lead implantation site is not known.
Methods: We performed a single center, retrospective cohort derivation study of 47 patients undergoing CRT implantation. Inclusion criteria included heart failure of ischemic etiology and availability of a high-rate venogram demonstrating a full heart cycle. The contraction amplitude was measured using venous landmarks. The primary end point was death or hospitalization for any cause.
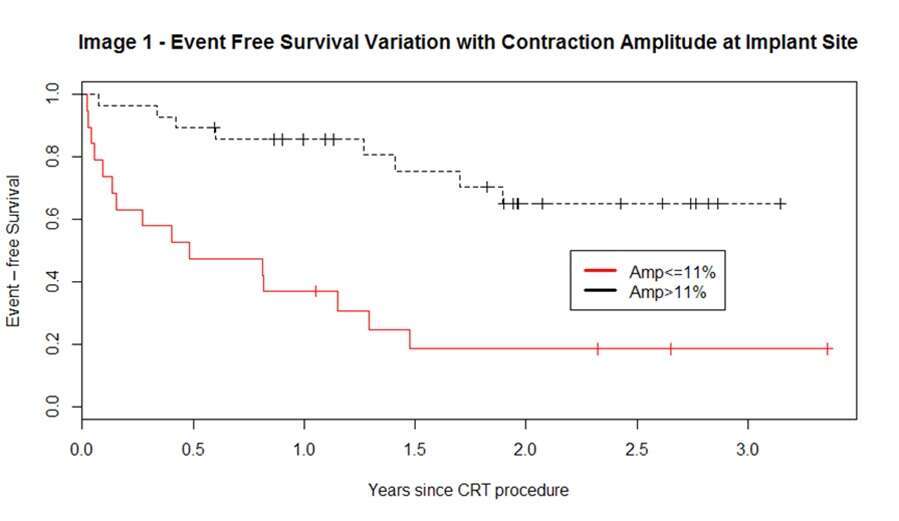
Results: 47 patients (85% male, mean age 69) were enrolled. 44 (94%) had ejection fraction <=35%. New York Heart Association (NYHA) class was II-III or higher in 44 (94%). 23 patients (49%) were hospitalized or died during a mean follow up period of 2.19 years. The event free survival rate for patients with pacing site amplitude above 11% (N=28) was significantly higher (image 1. Log rank p = 0.0001). Of 19 patients with low amplitude, 16 (84%) had alternative sites with amplitude above 11%.
Conclusion High contraction amplitude at the LV implant site, measured angiographically, is associated with improved outcome. Availability of strain measurements during CRT procedures may help avoid low-amplitude sites and achieve improved response.