Background
Current guidelines advocate immediate vs. early percutaneous coronary intervention (PCI) strategy in ST elevation vs. non ST elevation myocardial infarction (STEMI, NSTEMI).
There is however increasing concern that "next-day PCI" in NSTEMI may adversely affect LV systolic and/or diastolic function and a more urgent aggressive approach should be taken in NSTEMI, similar to that in STEMI.
In the current study we compared echocardiographic data between patients with STEMI and NSTEMI who had either primary or early PCI respectively.
Methods
Prospective data of 161 consecutive patients who presented with an acute MI was analyzed. Patients had primary PCI if they had STEMI and non-emergent PCI if they had NSTEMI.
Demographic, procedural times as well as post PCI echocardiographic left ventricular systolic and diastolic parameters were compared between STEMI and NSTEMI groups.
Results
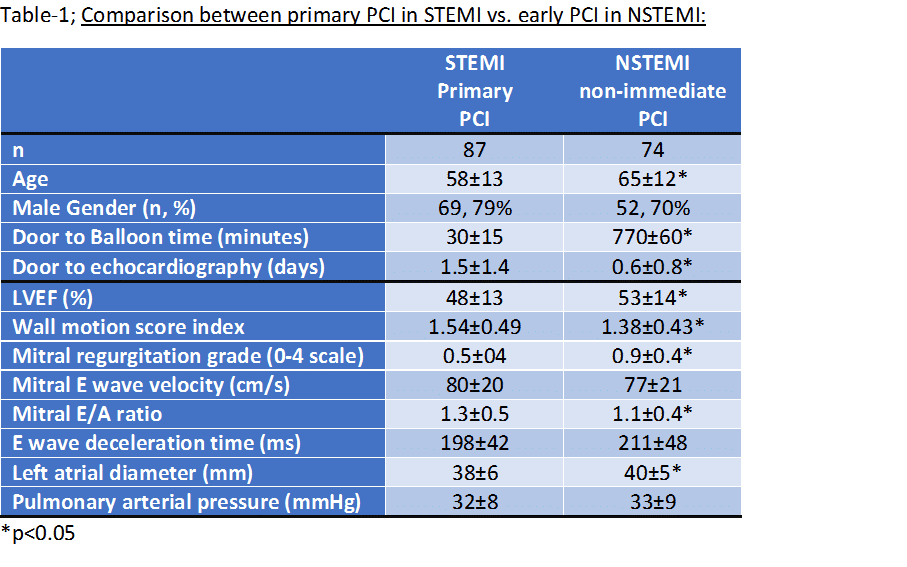
AS elaborated in Table-1, patients with STEMI were younger compared to patients with NSTEMI. Recorded time to intervention was significantly longer in NSTEMI, reflecting guideline derived intervention strategy (770±60 vs. 30±15min, for NSTEMI and STEMI, respectively, p<0.00001). Post interventional LV systolic function i.e. LV ejection fraction was better in NSTEMI compared to STEMI (53±14 vs. 48±13, respectively, p<0.05). Larger left atrial diameter and mild mitral regurgitation were more common in the NSTEMI patients while pulmonary arterial pressure was similar between the two groups.
Conclusion
Adherence to practice guidelines delaying PCI up to ~13hrs in patients with NSTEMI did not adversely affect left ventricular systolic and diastolic function compared to immediate PCI in patients with STEMI. Minor diastolic changes, most probably reflecting age differences between the groups, were present in NSTEMI patients. Based on current data, we conclude that early PCI intervention rather than an immediate one is appropriate in NSTEMI patients.